Def: A bacterial disease – of calcified tissues of teeth – involving demineralization of the inorganic structure – and destruction of organic substance – of the tooth.
Etiology of caries
1. Cariogenic bacteria:
- S. Mutans
- S. Sobrinus
- S. Oralis
- S. Sanguis
- S. Mitis
- Lactobacilli
- Actinomyces
2. Susceptible tooth surface
3. Substrate
4. Time
NB: Acidogenic Theory: W. D. Miller 1889
- Oral bacteria – ferment dietary CHO – form acid – decalcify tooth substance + destroy organic matrix
Experimental evidence: Role of S. Mutans in caries
1. Rapid generation of acid from sucrose
2. Synthesize extracellular polysaccharides
- To promote adhesion to tooth
- Increase plaque bulk
3. Synthesize intracellular polysaccharides – sustains acid production in the absence of sucrose
4. Present in high numbers in plaque associated lesions
5. Cariogenic and respond to immunizations in animal models
NB: This evidence is based on Koch’s postulates (1877)
- 1. Isolate organism from pt with dx
- 2. Culture organism outside the body
- 3. Organism can cause dx in healthy susceptible animals
- 4. Recover organism from inoculated animal. Pt’s serum contains antibodies to the organism.
NB:
- Gnotobites + Cariogenic diet: No caries
- Gnotobites + Cariogenic diet + Inoculated cariogenic bacteria: Caries develop
Etiology variables for caries progression
Intrinsic factors
Advantageous:
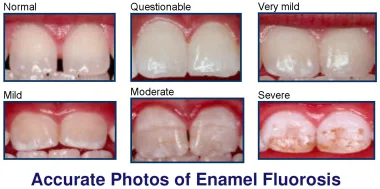
- Increased flouride conc. in enamel
- Decreased enamel solubility
Disadvantageous:
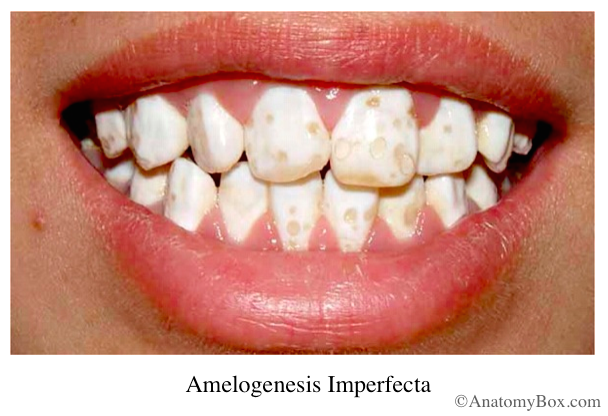
- Enamel hypoplasia and hypomineralization
- Deep pits and fissures
- Misaligned teeth
Extrinsic factors
1. Saliva
- Flow rate – High flow rate, decreased caries
- Viscosity – Low viscosity, increased caries
- Buffer (Ca2+ and Po42-)
- Antimicrobial agents – Immunoglobulins, lysozyme, lactoferrous, thiocyanates
2. Diet
- Presence of phosphates – Decreases caries
- Fat – Increases caries
- Trace elements (molybdenum, vanadium) – Decrease caries
Caries classification
1. Site of attack
- Pit/fissure caries
- Smooth surface caries
- Cemental/root caries
- Recurrent caries
2. Rate of attack
- Rampant/acute caries
- Slow/chronic caries
- Arrested caries
Factors affecting outcome of caries
1. Nature of irritant – Bacterial type and load
2. Duration and severity of irritant – Bacterial virulence
3. Amount of bacterial substrate
4. Apical blood flow
5. Local anatomy of pulp chamber
6. Pre-existing state of pulp
7. Extent of other trauma
8. Microbial factors – Pathogenicity is the ability of a microbial species to produce dx = Virulence
- Adhesion – Bacteria to tooth surface
- Invasiveness – Spread to host tissue after infection
- Toxigenecity – Endotoxin (cell wall), Exotoxin (excrete)
- Communicability – Spread from one host to another
9. Host defenses
– Local
- Epithelial lining – Physical barrier, IgA
- Saliva
- Colonization by normal flora
– Systemic
- Humoral immunity – Ig A, D, E, M, G
- Complement system & cytokines
- Cell immunity – Lymphocytes (B & T), PMN’s
Spread of microbes from dento-alveolar complex
- Direct invasion/extension
- Lymphatic
- Haematogenous
Histopathology of enamel caries
Ground sections of teeth examined by:
- Transmitted light
- Polarized light
- Microradiography
- Electron microscopy (Microdissected pieces of enamel)
- Biochemical studies (Microdissected pieces of enamel)
Phases of enamel caries:
- The early (submicroscopic) lesion
- Phase of non bacterial enamel crystal destruction
- Cavity formation
- Bacterial invasion of enamel
- Undermining of enamel from below after spread into dentine
Histological Zones:
NB: Due to absence of cellular sensors in enamel – there is no defense reaction
1. Surface zone: 40 um thick
- Little change in early lesion
- Highly mineralized: Fluoride and Magnesium
- Increased proteins
- Surface of enamel is resistant to acid attack due to its structure, therefore subsurface demineralization occurs
- Reprecipitation of minerals from:
- Plaque
- Minerals dissolved from deeper layers of lesion
2. Body of lesion: 2-25% pore volume
- Reprecipitation of minerals (from deeper zones) – form larger apatite crystals
- Continuous acid attack – more destruction of minerals – replaced by unbound water and organic matter from saliva and microbes
- Increased prominence of striae of Retzius: White spots
3. Dark zone: 2-4% pore volume
- Some remineralization concurrent with destruction
- Narrow zone: Rapidly advancing lesion
- Wide zone: Slow advancing lesion
- Reprecipitation occurs from translucent zone
4. Translucent zone: 1% pore volume = size of H2O molecule
- Normal enamel has 0.1% pore volume, therefore more porous than normal enamel
- 1st recognizable change at advancing edge of lesion
- Selective dissolution of Mg2+ and CO3-2 – Occurs at junctional areas btwn prismatic and interprismatic areas
NB: White spots stained with exogenous pigments (food, tobacco, bacteria) become brown spots
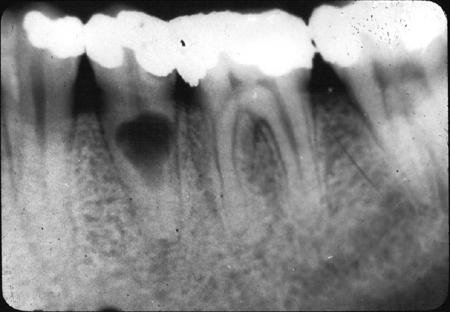
Histopathology of dentine caries
Defense reaction mediated by pulpo-dentinal complex
- Sclerosis
- Reactionary dentine
- Sealing of dead tracts
Caries destruction involves interacting processes
- Demineralization (acid always in advance of bacteria)
- Proteolysis of matrix
NB: Defense reaction of dentine may occur before caries reach dentine due to irritation of odontoblasts – tertiary dentine
NB: Circumpulpal dentine more resistant to carious attack due to increased F– diffused into from pulp
1. Zone of sclerosis (Translucent zone)
- Sclerosed dentine = Increased mineral content
- 2 patterns of mineralization:
- 1) Centripetal deposition of peritubular dentine – therefore occlude tubule
- 2) Minerals appear in cytoplasmic process of odontoblast – tubule occluded by odontoblastic processes
- Dead tracts: Opaque, seen in sclerotic zone
- Empty tubules + air + degraded odontoblastic processes
- Occluded at pulpal end of EBURNOID (thin layer of hyaline calcified material)
2. Zone of demineralization
- Wave of acid from bacteria in this zone
- No bacteria in this zone
3. Zone of bacterial invasion
- Bacteria multiply and extend within tubule
- Acidogenic organisms eg. lactobacilli – occupy tubules at periphery of lesion and produce acids
- Acidogenic + proteolytic organisms – attack demineralized matrix, therefore soften walls of tubules
Increased bacteria + Compression of inter and peritubular dentine = Break down of dentinal tubules – Liquefaction area (elliptical area)
The liquefaction areas are called liquefaction foci – which enlarge, increase in number and coalesce
4. Zone of destruction
- Cavitation at amelodentinal junction
- Transverse clefts (cracks) appear in dentine – perpendicular to the direction of dentinal tubules
- Contain bacteria and necrotic tissue
- Bacteria invade peri and intertubular dentine
5. Reactionary/Tertiary dentine
- Beneath lesion in pulp
- Pre-odontoblasts differentiate – lay down tertiary dentine to protect pulp
Histopathology of cementum caries
- Recession of gingiva – cementum exposed to oral environment – cementum more homogenous and laminated – therefore when attacked – caries produce saucer shaped lesions
- Prominent microbes:
- Strep. mutans
- Actinomycosis viscosus