Clinical appearance of enamel hypomineralization of systemic origin affecting one or more permanent first molars (PFM) that are frequently associated with incisors
Etiology:
- Oxygen shortage + low birth weight
- Parental risks – infection, maternal psychological stress
- Complications during delivery
- Respiratory diseases and oxygen shortage of ameloblasts
- Children born with poor general health
- Childhood febrile disease
Diagnosis:
- Demarcated opacities
- Post eruption breakdown
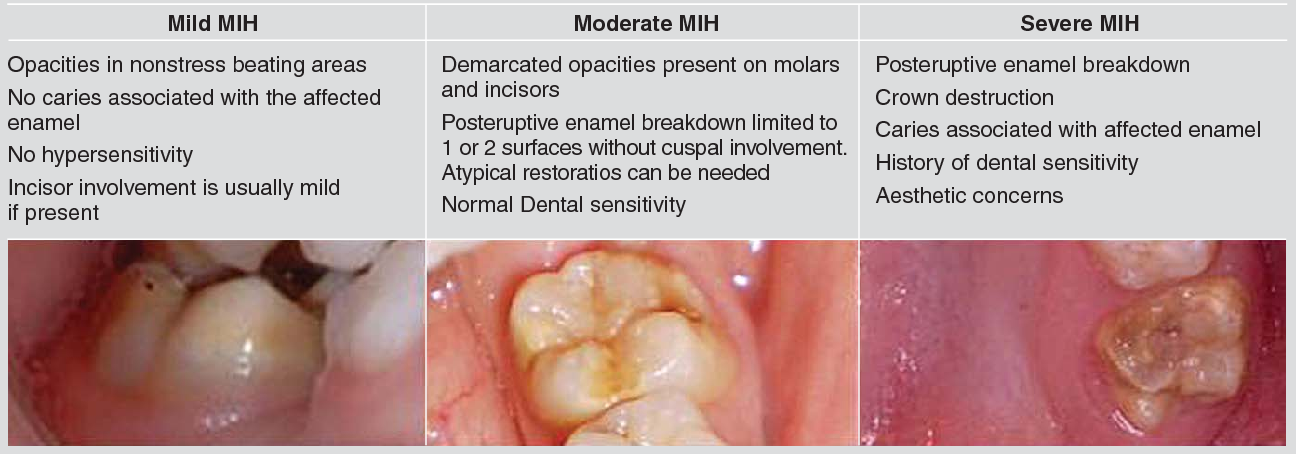
Criteria for MIH severity:
Differential diagnosis
- Enamel hypoplasia – Quantitative defect of decreased localized thickness of enamel
- Amelogenesis imperfecta
- Fluorosis
Challenges in treatment:
- Sensitivity and rapid development of caries
- Limited co-operation of a young child
- Difficulty achieving anesthesia – enamel is porous so exposed dentine results in chronic pulp inflammation
- Repeated marginal breakdown of restorations
Management:
- Early – Stainless steel crowns
- Moderate – Restoration
- Late – Extract PFM
- Fissure sealants
- Topical fluoride – toothpaste, fluoride varnish, fluoride gel
