
1) Tooth size
1. Microdontia
Teeth measurably smaller than normal
Clinical types:
- Absolute – smaller than normal
- Relative – gigantism
- Generalized – entire dentition
- Focal – usually 7’s & 8’s
Etiology:
- Genetic (AD) – Downs syndrome
- Irradiation therapy of 10 Gy or more
- Drawfism
- Congenital heart disease

2. Macrodontia
Enlarged teeth
Clinical types:
- Absolute – pituitary drawfism
- Relative – hypognathia of maxilla/ mandible
- Generalized – entire dentition
- Focal – some teeth eg. hemifacial hypertrophy

2) Tooth form
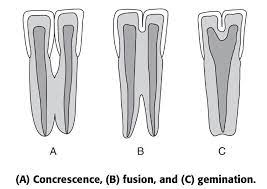
1. Double teeth
a) Germination – single enamel organ – 2 teeth develop
- 2 crowns share same root canal
- Aet: Trauma
b) Fusion – 2 tooth germs fuse by dentine ± pulp – forms single large tooth structure
- Aet: Trauma
c) Concrescence – adjacent formed teeth join by cementum
- Aet: Trauma, overcrowding
d) Twinning – Mirror image teeth. Complete germination
- One tooth germ – develops into 2 teeth
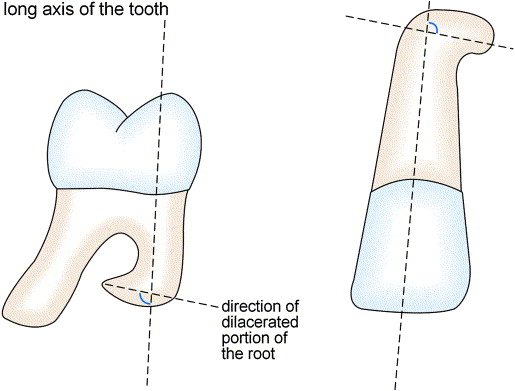
2. Dilaceration
Bending of roots at an angle at long axis of tooth
- Aet: Trauma during root development
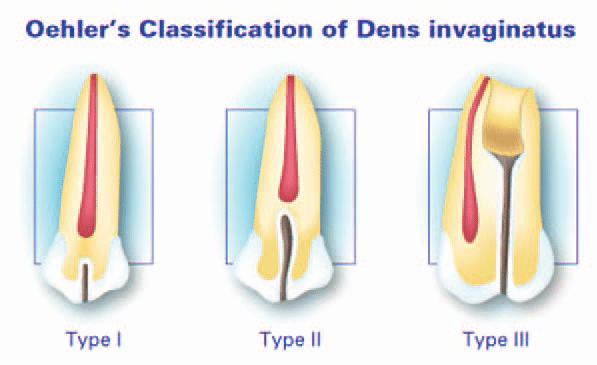
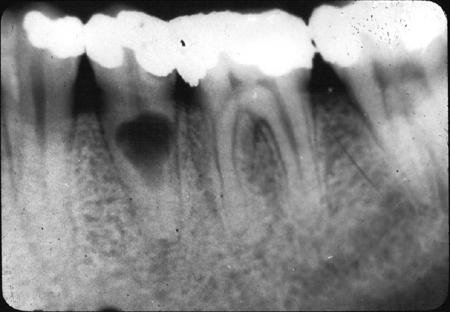
3. Dens invaginatus
Abnormal exaggeration of lingual pit
- Type I:
- Enamel lined cavity confined to tooth crown, not extending beyond CEJ
- Mx: Pit sealing
- Type II:
- Enamel lined cavity into tooth (± communication with pulp)
- Mx: XLA
- Type III:
- Invagination extends beyond CEJ
- Perforating apically or laterally at a foramen (no pulpal communication)
- Mx: XLA
4. Dens evaginatus
Anomalous tubercle/ cusp projecting from occlusal surface – usually premolar
- Extra cusp worn down, predispose to tooth decay

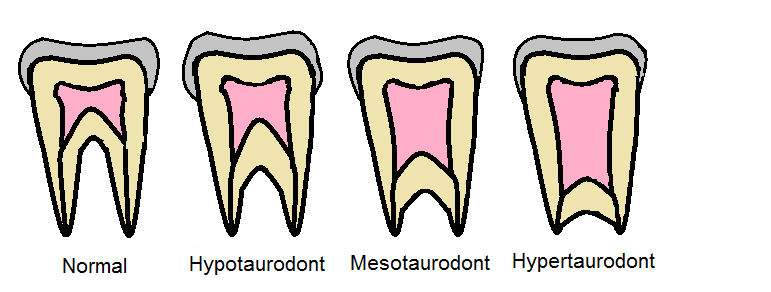
5. Taurodontism
Bull teeth
- Elongated crowns with increased apico-occlusal height of pulp chambers
- Failure of Hertwig’s root sheath to invaginate at proper horizontal level
6. Talon cusp/ talon cingulum
Exaggeration of cusp shaped cingulum esp. Max. anteriors
- Mx: Fissure sealing & pulpotomy

7. Transposition
One tooth in place of another

8. Supernumerary
- Roots: Mand. canine, premolar, molar (8)
- Cusps:
- Cusp of carabelli
- Enamel pearl (root furcation)
- Dens evaginatus
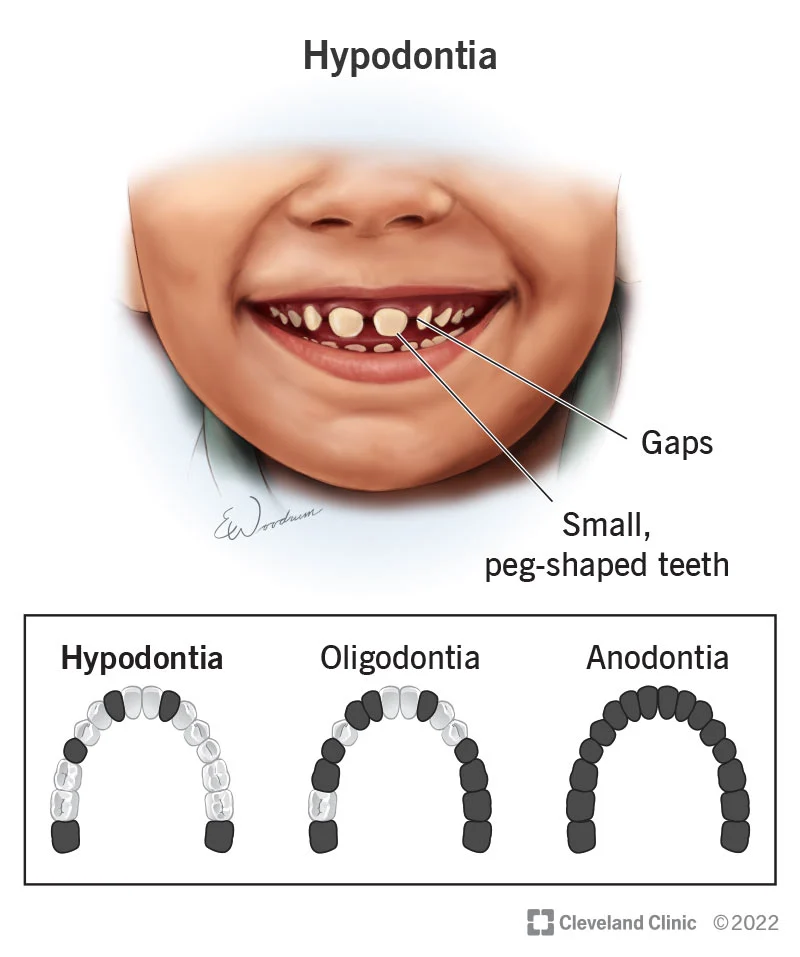
3) Tooth number
1. Anodontia
Absence of teeth
- Complete
- Partial:
- Hypodontia (<6 teeth)
- Oligodontia (>6 teeth)
- Aet:
- 1. Failure to form dental lamina
- 2. Failure to develop tooth buds
- 3. Premature breakdown of dental lamina
- 4. Autosomal dominant inheritance
- High prevalence in:
- Females
- Hereditary ectodermal dysplasia
- Orofacial cleft
- Down’s syndrome
Hereditary Ectodermal dysplasia
- X – Linked recessive
- Nail dystrophy
- Hypotrichosis
- Hyperkeratosis
- Oligodontia
2. Pseudodontia
Clinical absence of teeth
Aet:
- Impaction
- Delayed eruption
3. False anodontia
Teeth exfoliated or extracted
4. Hyperdontia
Excess teeth
- Supplemental – Normal dental series
- Supernumerary – Abnormal morphology
- Mesiodens – In maxillary midline
- Paramolar/ distodens – 4th molar
- Natal – Present at birth
- Neonatal – Immediately after birth (30 days)


Syndromes associated with hyperdontia
- Multiple supernumeraries
- Aplasia of one or both clavicle
- Delayed closure of fontanelles & sutures
- Wormian bones in suture lines
- Short sagittal diameter of cranial base
- Large transverse diameter of cranium
- Multiple unerupted supernumeraries & dentigerous cysts
- Multiple osteomas of facial bones
- Multiple adenomatous polyposis of colon
- Desmoid tumors
- Cutaneous epidermoid cyst
- Fibrous hyperplasia of skin & mesentery
4) Tooth colour
1. Extrinsic staining
Not incorporated into tooth substance
- Chromogenic bacteria (green, black, yellow orange)
- Restorative materials:
- Silver amalgam (gray black)
- Resins (yellow brown)
2. Intrinsic staining
Incorporated into tooth structure
Changes in structure/ thickness of dental tissues:
- Enamel hypoplasia
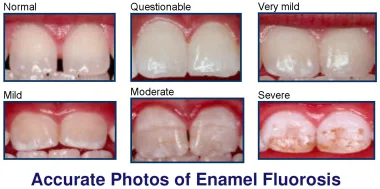
- Fluorosis
- Caries
- Dentine dysplasia II
- Amelogenesis imperfecta
- Dentinogenesis imperfecta
- Enamel opacity
- Age changes
Diffusion of pigments during/ after dental development:
- Tetracycline – cross placental barrier – yellow/ grey, brown
- Bilirubin – green/ brown
- Liver disease/ neonatal hepatitis – Yellow brown
- Porphyrins
- Pulp necrosis products
- RH incompatibility (erythroblastosis fetalis)
- Endodontic materials
5) Tooth eruption
1. Accelerated eruption
Symmetrical:
- Adrogenital syndrome
- Cerebral gigantism
Unilateral:
- Facial hemihypertrophy
- Sturge – Weber syndrome
- Vascular anomalies of bone (+ macrodontia)
2. Delayed eruption
Symmetrical:
- Congenital hypothyroidism/ hypopituitarism
- Cleidocranial dysplasia
- Downs syndrome
Unilateral:
- Regional odontodysplasia
- Ankylosing of primary predecessor
- Dilaceration
- Severe enamel hypoplasia:
- Nutritional deficiancy
- Traumatic displacement of tooth germs
- Obstruction by impaction:
- Rare in 1ry teeth, except 1st molar – Ankylosis/ submergence
- Multiple impactions – Cleidocranial dysplasia
- Single impaction:
- Supernumeraries
- Odontomes
- Cysts
- Crowding
3. Reimpaction of teeth
Previously erupted tooth becomes submerged in tissues
Aet:
- Deficient development of alveolar process
- Root ankylosed + Lack of growth of alveolar process
4. Premature loss
- Juvenile & prepubertal periodontitis
- Hypophosphatasia
- Leukemia
- Chronic neutropenia
- Acrodynia (pink disease) – Hg poisoning
- Dental caries
- Hereditary palmer – planter hyperkeratosis
- Langerhans cell histiocytosis – proliferation of abnormal histiocytes
- Tooth mobility
- Floating teeth in multiple quadrants
- DI
- Short stature
- Neurosensory deafness
5. Prolonged retention
Deciduous teeth not shed
- Mand 1’s – Lingual eruption esp. Down’s syndrome
- Max 6’s – Path of eruption further anterior than normal
6. Occlusal defects
- Deep/ increased overbite:
- Over eruption of ant. teeth
- Infra eruption of post. teeth
- Open bite:
- Usually ant. region
- Post. mandibular growth disorder
- Macroglossia
6) Degenerative changes (acquired)
1. Attrition
- Physiologic wearing of teeth due to mastication
- Abnormal occlusion habits: bruxism, tobacco/ betel chewing, abnormal tooth structure (AI, DI)
- Histology: Reactionary dentine, dead tracts, translucent zones

2. Abrasion
- Pathologic wear of teeth – abnormal habit, abnormal use of abrasives orally
- Eg. Pipe smoking, tobacco chewing, aggressive tooth brushing, abrasive dentifrices, pins & nails (carpenters)

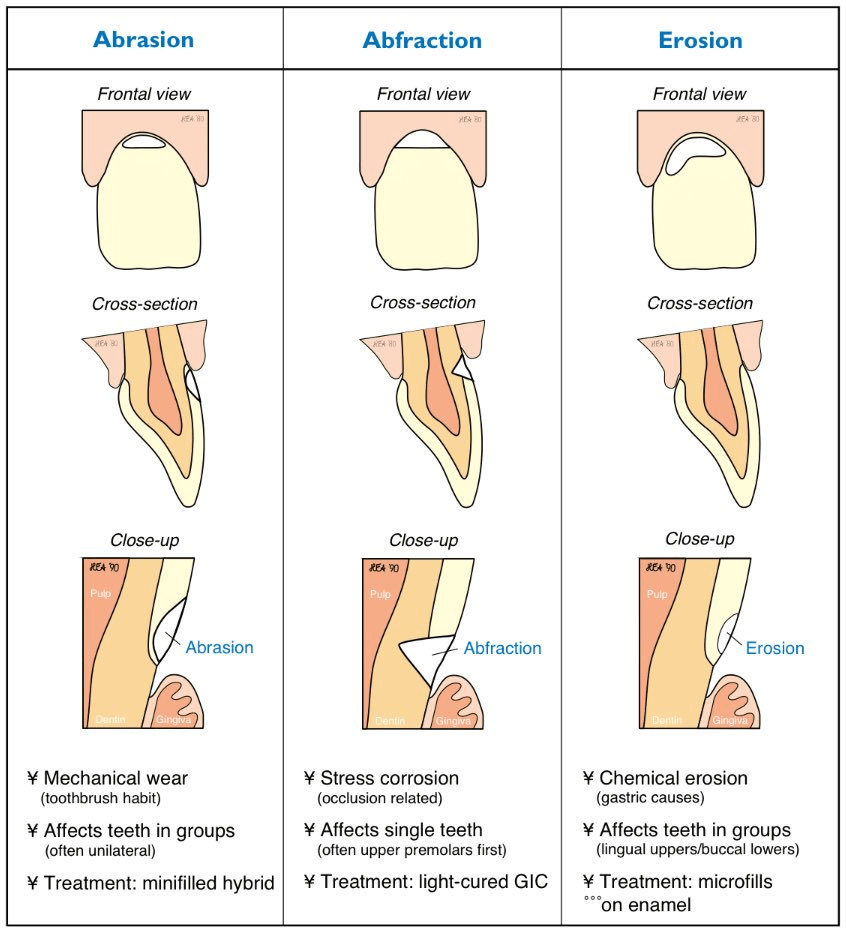
3. Erosion
- Loss of tooth substance due to non-bacterial chemical process:
- Occupational – car battery acid
- Dietary – acidic drinks
- Chronic vomiting – anorexia, bulimia

4. Resorption
- Physiological – shed deciduous teeth
- Pathological:
- Periapical inflammation
- Iatrogenic – excess orthodontic force
- Neoplasms
- Impacted teeth
- Transplanted/replanted teeth
- Idiopathic
- External resorption: 2ry to pathology (or idiopathic)
- Internal resorption: 2ry to pulpitis (or idiopathic)
7) Tooth structure
A) Enamel
1. Enamel hypoplasia
- Quantitatively defective – ameloblast fail to produce normal volume of matrix
- Enamel normal hardness
- Clinical:
- Pit/ grooves on enamel surface
- General decrease in enamel thickness
- Ground section: Decreased prisms than normal + abnormal direction
2. Enamel hypocalcification
- Qualitatively defective – hypomineralized
- Normal amounts of enamel
- Clinical:
- White & opaque – after eruption – orange brown
- Quickly chips off & wears off
- Ground section: Surface layers = normal
Classification
1. Local causes
- Trauma
- Irradiation
- Infection – single tooth
- eg. Turner’s tooth – hypocalcified permanent tooth due to abscess overlying deciduous tooth (yellow/ brown)
- Idiopathic (enamel opacities) – hypocalcification of 1ry & 2ry teeth esp. 11 and 21
2. Generalized causes
a) Environmental (chronological hypoplasia)
Birth to 6 years ie. period of crown formation of permanent teeth – ameloblast dysfunction
- Prenatal:
- Maternal disease
- Rubella
- Syphilis (T. pallidum):
- Hutchinson’s incisors – tapered crown + notched incisal edge
- Mulberry molars – Lobulated occlusal surfaces
- Neonatal:
- Hemolytic disease of new born
- Prolonged labour
- Premature birth
- Hypocalcemia:
- Hypercalcemia:
NB: Disorders in calcium metabolism cause dysfunction of ameloblasts
- Postnatal:
- Measles
- Chicken pox
- Scarlet fever
- Whooping cough
- Pneumonia
- Congenital heart disease
- GIT disease
- Hyperparathyroidism
- Fluorosis – > 1ppm, incorporates into maturation stage (not in utero due to placental barrier)
- Vitamin A, C, D deficiency
- Rickets
b) Genetic
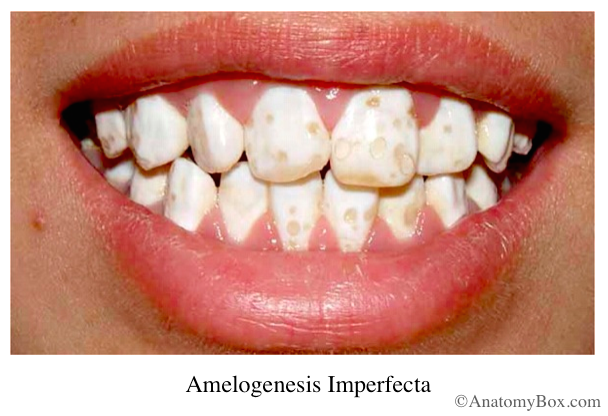
Only teeth affected: Amelogenesis imperfecta
- Mutation on distal short arm of x chromosome – codes for amelogenin protein
- Classification:
- 1. Hypoplastic:
- Areas of tooth enamel fail to form normal contour
- Enamel is normal hardness but thin
- Sharp needle like cusps/ pitting/ vertical grooving & wrinkling
- Yellow + gross attrition with time
- 2. Hypomaturation:
- Enamel of normal thickness but wears away easily
- 3. Hypocalcified:
- Soft enamel lost easily after eruption
- Yellow – brown plus gross attrition
- Chalky consistence – Chips off
- 1. Hypoplastic:
Teeth + generalized disease:
- Ectodermal dysplasia
- Down’s syndrome
- Epidermolysis
B) Dentine
1. Dentinogenesis imperfecta (hereditary opalescent dentine)
- Autosomal dominant (AD)
- Mutations in structural genes for collagen type 1
- Therefore occur with osteogenesis imperfecta
- On eruption – normal contour but opalescent amber like appearance – becomes translucent + grey/brown + bluish reflection from enamel
- Rapidly lost attrition
- Radiological:
- Short, blunt roots
- Partial/ total obliteration of pulp chamber & root canal by dentine
- Histology:
- Normal mantle dentine
- Decreased tubules – wide & irregular
- Straight DEJ (not scalloped)
- Vascular inclusions in dentine – remnants of odontoblasts + pulp tissue
- Biochemical:
- Increased water content
- Decreased mineral content
- Decreased microhardness
- Classification:
| I | II | III | IV |
| AD | AD | AD | AR |
| Opalescent dentine in 1ry & 2ry | Discoloured teeth | Opalescent teeth | Brown opalescent teeth |
| White sclera | Blue sclera | Blue/ white sclera | White sclera |
| Bone fragility | Bone fragility Severe long bone deformity | Rapid dentine abrasion Severe bone fragility Skeletal deformity Growth retardation |
2. Shell teeth
- Rare
- Homozygote form of DI – No pulp chamber obliteration
- Thin dentine, forms shell around pulp
- Short roots
3. Dentinal dysplasia (rootless teeth)
- Rare AD
- Normal crown + dysplastic dentine in roots having many calcified, spherical bodies
- Obliterated root canals & pulp chamber
- Roots are stunted
2 types caused by fragmentation of Hertwig’s root sheath:
- Radicular DD:
- Abnormal root formation
- Periapical resorption
- Therefore teeth exfoliate prematurely
- X-ray: Short roots & obliterated pulp
- Coronal DD:
- Discolouration of 1ry teeth
- Obliteration of pulp chamber
- Distorted crowns of permanent teeth
- X-ray: Enlarged pulp chambers
NB: Metabolic disturbances affecting dentinogenesis:
- Rickets
- Vitamin D resistant rickets
- Hypophosphatasia
- Dentine dysplasia I & II
4. Regional odontodysplasia (enamel & dentine defect)
- Involves ectodermal (enamel) & mesodermal (dentine + cementum)
- Results from disorderly proliferation of dental epithelium at an early stage – of formation of hard tissues – in each affected
- Etiology: Local vascular deficiency during tooth development
- Clinical:
- Delayed eruption
- Irregular shape – hypoplastic and irregularly mineralized enamel
- Dentine – thin + large interglobular dentine
- Affects a region/ quadrant of maxilla/ mandible
- Usually anterior maxilla and unilateral
- X-ray:
- Ghost teeth
- Decreased radiopacity
- Loss of distinction between enamel and dentine
- Histology:
- Abnormal odontogenic epithelial cells
- Abnormal globular dentine

C) Cementum
1. Hypercementosis
Increased cementum deposition
Etiology:
- Root ankylosis & concrescence
- Periapical inflammation – Localized knob-like enlargement
- Mechanical stimulation – Below threshold cementum deposition, above threshold bone resorption
- Functionless teeth – Resorption + increased opposition
- Unerupted teeth – If no REE – cementum over extends surface of enamel
- Paget’s disease – Irregular masses and ankylosis
- Idiopathic
REE – Reduced enamel epithelium – lies over developing tooth

2. Hypoplasia & dysplasia
- Cleidocranial dysostosis (mentioned above)
- Hypophosphatasia – aplasia of cementum (AR disease)

5 thoughts on “Odontodysmorphogenesis”
Comments are closed.