Silk road disease
Etiology:
- Autoimmune – multisystemic disease
- Human leukocyte antigen HLA-B51
Clinical:
- Recurrent orogenital ulcers
- Pustular skin lesions
- Ocular complications
Silk road disease

Genetic disorder – Premature fusion of certain skull bones (craniosynostosis) – skull does not grow normally – affects shape of head and face
1. Skeletal abnormalities:
2. Oral complications:
3. Ovoid skull + horizontal supra-orbital groove
4. Early closure of coronal & sagittal sutures
Surgery

Triad:

Thanatophoric dwarfism – Missense/ point mutation in FGFR3. Fatal

Teeth measurably smaller than normal
Clinical types:
Etiology:

Enlarged teeth
Clinical types:

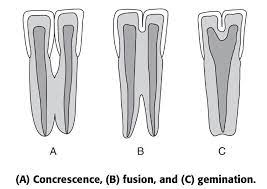
a) Germination – single enamel organ – 2 teeth develop
b) Fusion – 2 tooth germs fuse by dentine ± pulp – forms single large tooth structure
c) Concrescence – adjacent formed teeth join by cementum
d) Twinning – Mirror image teeth. Complete germination
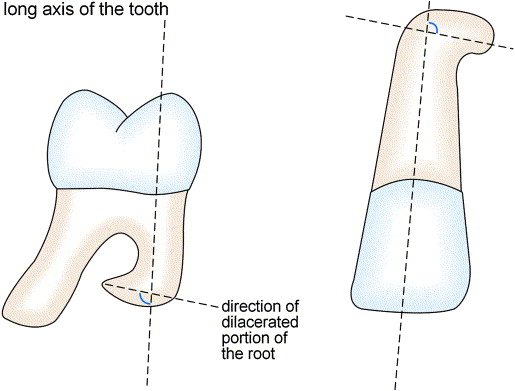
Bending of roots at an angle at long axis of tooth
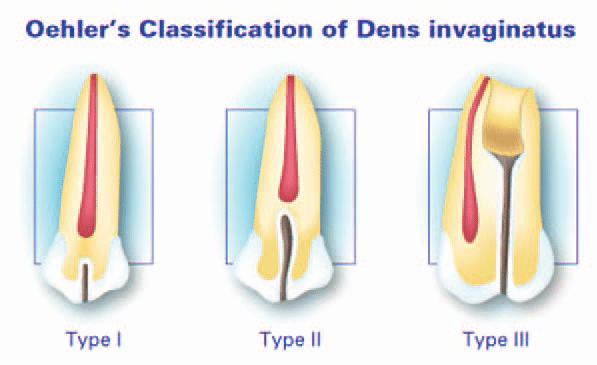
Abnormal exaggeration of lingual pit
Anomalous tubercle/ cusp projecting from occlusal surface – usually premolar

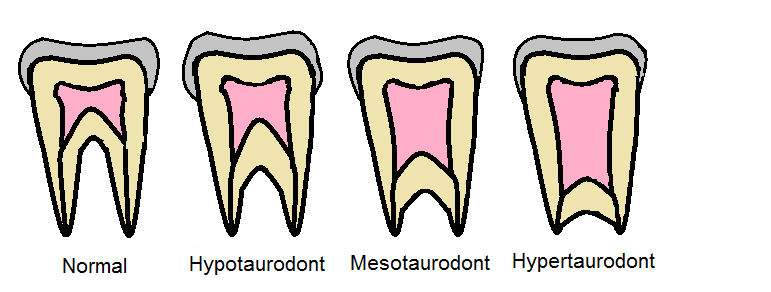
Bull teeth
Exaggeration of cusp shaped cingulum esp. Max. anteriors

One tooth in place of another

Absence of teeth
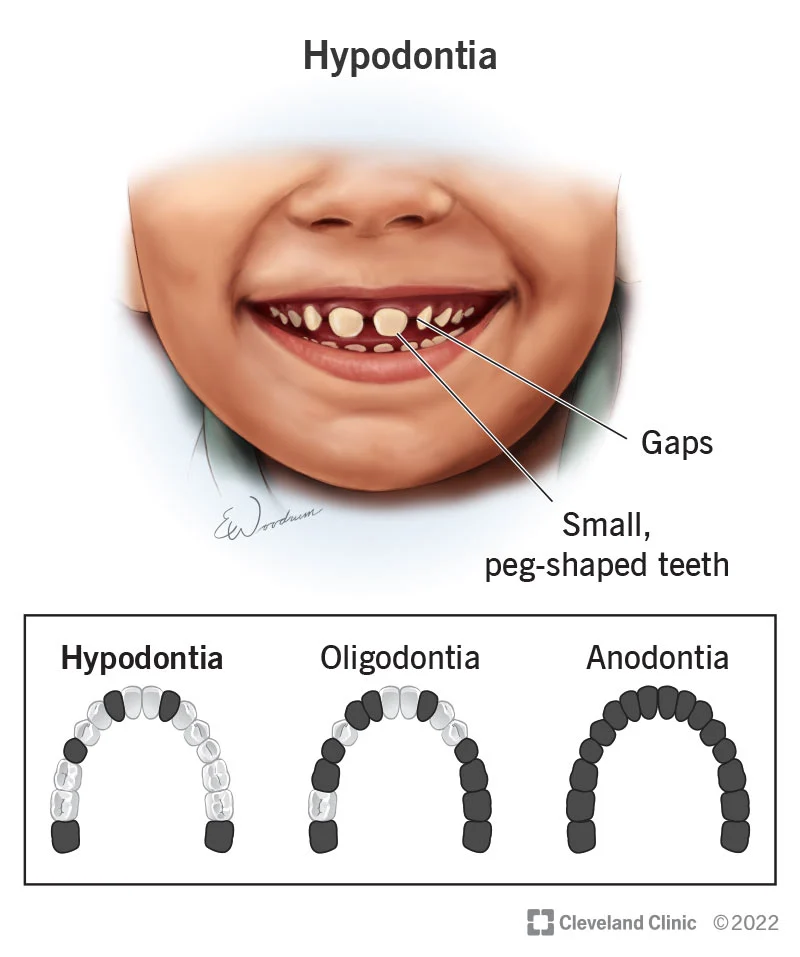
Clinical absence of teeth
Aet:
Teeth exfoliated or extracted
Excess teeth


Not incorporated into tooth substance
Incorporated into tooth structure
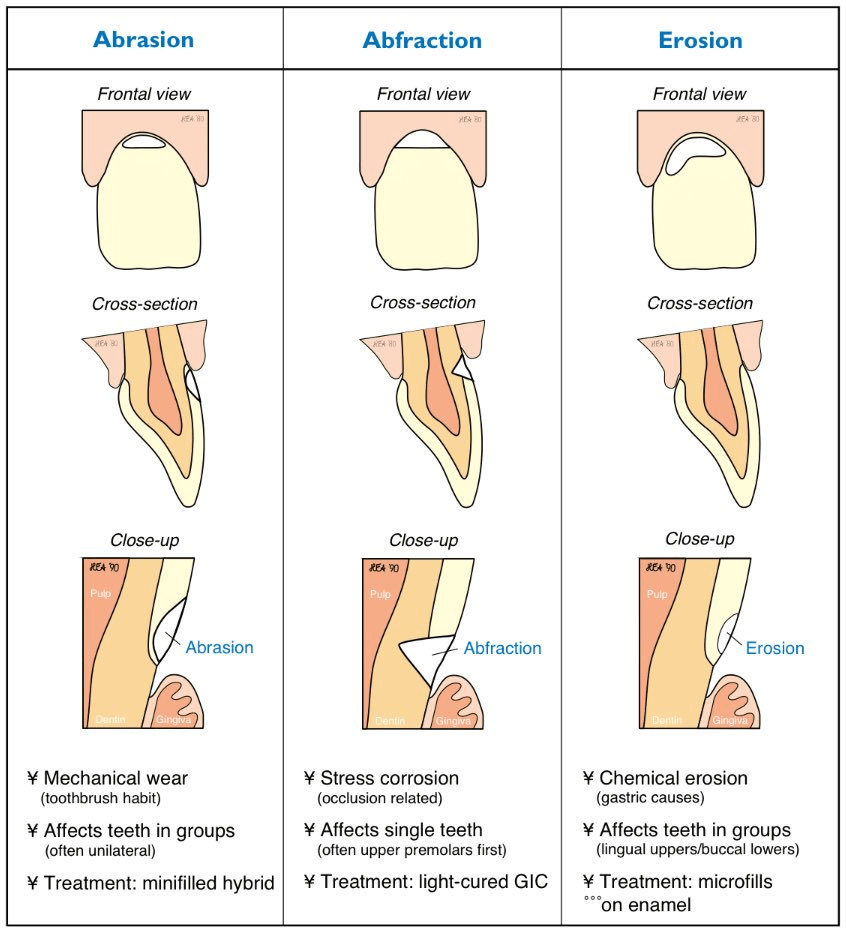
Changes in structure/ thickness of dental tissues:
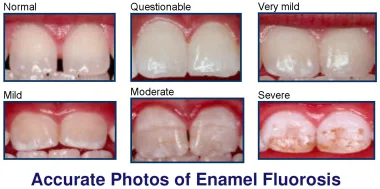
Diffusion of pigments during/ after dental development:
Symmetrical:
Unilateral:
Symmetrical:
Unilateral:
Previously erupted tooth becomes submerged in tissues
Aet:
Deciduous teeth not shed



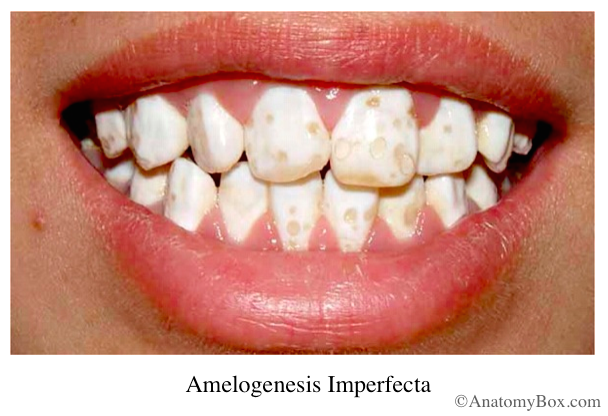
Birth to 6 years ie. period of crown formation of permanent teeth – ameloblast dysfunction
NB: Disorders in calcium metabolism cause dysfunction of ameloblasts
Only teeth affected: Amelogenesis imperfecta
Teeth + generalized disease:
| I | II | III | IV |
| AD | AD | AD | AR |
| Opalescent dentine in 1ry & 2ry | Discoloured teeth | Opalescent teeth | Brown opalescent teeth |
| White sclera | Blue sclera | Blue/ white sclera | White sclera |
| Bone fragility | Bone fragility Severe long bone deformity | Rapid dentine abrasion Severe bone fragility Skeletal deformity Growth retardation |
2 types caused by fragmentation of Hertwig’s root sheath:
NB: Metabolic disturbances affecting dentinogenesis:

Increased cementum deposition
Etiology:
REE – Reduced enamel epithelium – lies over developing tooth

Def: Inflammation of gingiva without clinical attachment loss
1. Dental plaque induced gingival disease
2. Non plaque induced gingival lesion
Def: Aggregate of microorganisms – in which cells produce extracellular matrix – and are adherent to each other – and onto the tooth surface
Steps on plaque formation:
Risk factors:
1. Intrinsic
2. External/acquired
3. Local
Factors contributing to severity:
Def: Inflammation of supporting tissues of the teeth with clinical attachment loss
1. Prepubertal (accelerated) periodontitis – Rare, genetic/medical condition
2. Juvenile Periodontitis – Uncommon, puberty & adolescence
3. Rapidly progressive/ aggressive – Uncommon, late adolescence
4. Chronic adult periodontitis – Common, adults over 30
*Cause gingival hyperplasia
| Healthy gingiva | Chronic gingivitis | Chronic periodontitis | |
| Aerobes : Fac. anaerobes | 75 : 25 | 60 : 40 | 20 : 80 |
| G+ve : G-ve | 90 : 10 | 65 : 35 | 25 : 75 |
| Motile : Non motile | 1 : 40 | ↑ motility rods & spirochetes | Abundant motile rods & spirochetes |
| Main species | Streptococcus Actinomyces Veilonella | S, A, V Capnocytophaga Fusobacteria Prevotella Porphyromonas | A, F, P, P Camphylobacter Eikenella |
Progression depends on balance between host & microbial factors
Host factors:
Microbial factors:
1. Initial lesion: 2-4 days, base of gingival sulcus. Gingivitis
2. Early lesion: 4-7 days, exacerbation of initial gingivitis
3. Established lesion: 2-3 weeks, disrupt JE. Gingivitis
4. Advanced lesion: Periodontitis – 3 weeks – inflammation spreads to alveolar bone & PDL
– Mechanism of degradation of CT and collagen:
– Pathological features of established PDL disease:
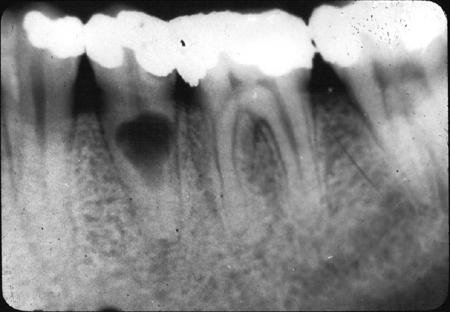
Apical periodontitis: Tender on mastication, edema and inflammation in pdl. Widened pdl due to bone resorption in x-ray.

Localized area of pus in PDL pocket
Acute pericoronitis – Common site – 7 & 8
Disease of young people
Etiology:
Clinical presentation:
Predisposing feature:
Etiology:
Underlying systematic disease:
Clinical presentation:
Complication:
Management:
Clinical presentation:
Histology:
Management:
1. Periapical osteitis – Localized inflammation of bone marrow spaces. Throbbing pain and tenderness to vertical percussion.
2. Phoenix abscess – Acute inflammation superimposed on a chronic lesion eg. cyst or granuloma
3. Pericoronitis – Infection of soft tissues (operculum) surrounding the crown of a partially erupted tooth
4. Folliculitis – Infection of follicle of developing 2ry teeth (spreads from 1ry predecessors)
5. Fistula – Abscess communicates with an epithelial surface
6. Ludwig’s angina – Rapidly spreading – septic cellulitis – involving submental, submandibular & sublingual spaces bilaterally
NB:
Primary fascial spaces: Adjacent to origin of infection
Secondary fascial spaces:
| Abscess | Cellulitis |
| Localized collection of pus | Inflammation of CT, non suppurative |
| Pocket with necrotic tissue, bacterial colonies and dead white cells | Warm, diffuse, erythematous, indurated tissue in infected area |
| Chronic | Acute |
| Localized pain | Severe and generalized pain |
| Well circumscribed | Diffuse |
| Fluctuant | Indurated |
| Anaerobic | Aerobic |
1. Chronic dento-alveolar abscess – Abscess from dental tissues spreads into alveolar bone. Sinus through alveolar bone onto mucosa near level of apex. Tender on percussion, no EPT response, Ice relieves pain, heat aggravates. Management: Drainage via pulp chamber/trephination, irrigate with H2O2 and normal saline, antibiotics
2. Condensing osteitis – Deposition of bone along existing trabeculae due to chronic irritation
3. Osteosclerosis – Deposit compact bone within trabecular area
4. Granuloma – mass of granulation tissue, consists of:
5. Periapical scar – Dense fibrous tissue. Scar forms after periapical inflammation resolves
6. Periostitis – Inflammation of periosteum (Vascular CT enveloping bones)
7. Hypercementosis – Excessive deposition of cementum
8. Osteomyelitis – Bone marrow infection
1. Intracanal spread by septic emboli
3. Bacteremia – detectable levels of bacteria in blood
4. Septicemia – Increased bacteria + toxins in blood
5. Septic shock – Septicemia, G-ve bacteria, inadequate perfusion of tissues
Untreated dental infections can lead to:
A) Local:
B) Systemic (ascending):
C) Systemic (descending):
Def: A bacterial disease – of calcified tissues of teeth – involving demineralization of the inorganic structure – and destruction of organic substance – of the tooth.
1. Cariogenic bacteria:
2. Susceptible tooth surface
3. Substrate
4. Time
NB: Acidogenic Theory: W. D. Miller 1889
1. Rapid generation of acid from sucrose
2. Synthesize extracellular polysaccharides
3. Synthesize intracellular polysaccharides – sustains acid production in the absence of sucrose
4. Present in high numbers in plaque associated lesions
5. Cariogenic and respond to immunizations in animal models
NB: This evidence is based on Koch’s postulates (1877)
NB:
Intrinsic factors
Advantageous:
Disadvantageous:
Extrinsic factors
1. Saliva
2. Diet
1. Site of attack
2. Rate of attack
1. Nature of irritant – Bacterial type and load
2. Duration and severity of irritant – Bacterial virulence
3. Amount of bacterial substrate
4. Apical blood flow
5. Local anatomy of pulp chamber
6. Pre-existing state of pulp
7. Extent of other trauma
8. Microbial factors – Pathogenicity is the ability of a microbial species to produce dx = Virulence
9. Host defenses
– Local
– Systemic
Ground sections of teeth examined by:
Phases of enamel caries:
Histological Zones:

NB: Due to absence of cellular sensors in enamel – there is no defense reaction
1. Surface zone: 40 um thick
2. Body of lesion: 2-25% pore volume
3. Dark zone: 2-4% pore volume
4. Translucent zone: 1% pore volume = size of H2O molecule
NB: White spots stained with exogenous pigments (food, tobacco, bacteria) become brown spots
Defense reaction mediated by pulpo-dentinal complex
Caries destruction involves interacting processes
NB: Defense reaction of dentine may occur before caries reach dentine due to irritation of odontoblasts – tertiary dentine
NB: Circumpulpal dentine more resistant to carious attack due to increased F– diffused into from pulp

1. Zone of sclerosis (Translucent zone)
2. Zone of demineralization
3. Zone of bacterial invasion
Increased bacteria + Compression of inter and peritubular dentine = Break down of dentinal tubules – Liquefaction area (elliptical area)
The liquefaction areas are called liquefaction foci – which enlarge, increase in number and coalesce

4. Zone of destruction
5. Reactionary/Tertiary dentine
1. Plain Radiograph
2. Contrast Radiograph – Radiopaque substance introduced in body
Sialography:
– Iodine
Angiography
TMJ arthroscopy
Radionuclide imaging
3. Digital Imaging – Receptor converts x-ray image into digital data and stores on computer
4. Conventional Tomography – Greater range of movement, image tissues in slices
5. Computed Tomography (CT Scan)
6. MRI
7. Positron Emission Tomography (PET) – Radiation/nuclear medicine to produce 3D colour image
8. Ultrasonography
1. Haematology
EDTA:
Plain Tube:
Citrated Tube:
2. Biopsy – Histopathology
3. Microbiology – Culture and sensitivity
NB: Don’t take samples for viral hepatitis and HIV, refer to VCT clinic
1. Light Microscopy
2. Electron Microscopy: Resolution of small microbes (virology)
a) Gram Stain – Lugol’s iodine, carbolfuchsin
b) Ziehl – Nielsen – Carbolfuchsin + methylene blue/ malachite green
a) MacConkey
b) Mitis Salivarius
c) Mannitol Salt
d) Lowenstein – Jensen
e) TCBS (Thiosulphate, citrate, bile, saliva)
f) Thayer Martin
g) Charcoal Yeast
Stuart transport media (semi – solid, non nutrient agar)