Arteries

(I) Abdominal aorta:
- Lower border of T12 – lower border of L4 (aortic hiatus to bifurcation)
- Travels down posterior wall of abdomen
- Runs on the left and parallel to IVC
- At L4 bifurcates
Relations:
- Anterior – Lesser omentum, stomach, pancreas
- Posterior – Vertebral column, lumbar veins
- Right – IVC, azygos vein, cisterna chyli, right crus diaphragm
- Left – Left crus diaphragm, ascending duodenum, small intestines
Clinicals:
- Rupture of abdominal aortic aneurysm – deep pain in abdomen, back pain, hemoperitoneum (blood in peritoneal cavity) – leads to hemorrhagic shock – rapid death
(II) Celiac trunk:
- 1st branch of abdominal aorta – T12
- Divides into 3 branches
(III) Superior mesenteric artery:
- 2nd branch of abdominal aorta – L1
- Posterior to neck of pancreas
- Pass between pancreas head and uncinate process
- Terminates in right iliac fossa as ileocolic artery
(IV) Inferior mesenteric artery:
- 3rd branch of abdominal aorta – L3
- Posterior to left psoas major
- Terminates as superior rectal artery
Clinicals:
- Peptic ulcers – erode gastroduodenal artery, leads to gastrointestinal bleeding
- Celiac trunk compression syndrome – due to median arcuate ligament, leads to ischemia (median arcuate ligament connects right and left crura of diaphragm)
- Splenic artery aneurysm
- Left hemicolectomy – surgical removal of descending colon – dissect branches of IMA and IMV
Veins

(I) IVC:
- Formed by left and right common iliac veins at L5
- Ascends on right of vertebral column and aorta
- Anterior to right psoas major
- Grooves liver
- Enters through diaphragm at T8 – caval opening
Relations:
- Anterior – Head of pancreas, epiploic foramen, right and caudate lobe liver
- Posterior – Right psoas major, right crus diaphragm, Lower lumbar vertebrae
- Right – Right kidney, right lobe liver
- Left – Abdominal aorta
(II) IVC and SVC communication sites:
1. Thoracoepigastric – connects lateral thoracic vein (axillary vein – SVC) and superficial epigastric vein (femoral vein – IVC)
2. Superior epigastric (internal thoracic – SVC) and inferior epigastric (external iliac – IVC)
3. Azygos venous system
4. Vertebral venous plexus – Lumbar veins (IVC) and posterior intercostal veins (SVC)
(III) Portal vein:
- Formed from superior mesenteric vein and splenic vein – behind neck of pancreas
- Before reaching liver, portal vein divides into right and left branches – divides in to smaller venous branches
- Drains into hepatic sinusoids (supply blood to liver)
Clinicals:
- Portal hypertention – obstruction of blood flow through portal system, blood redirected through portosystematic anastomosis, veins become dilated – varices and hemorrhoids
- Infection of portal vein (pylephlebitis)
Nerves
(I) Nerves of abdominal wall: Somatic – Parietal peritoneum and skin
1. Anterolateral abdominal wall: Anterior rami of:
- T7-T9 – Skin superior to umbilicus
- T10 – Skin around umbilicus
- T11 – Skin inferior to umbilicus
- T12/Subcostal – Skin inferior to umbilicus
- L1 – Iliohypogastric and ilioinguinal – Skin inferior to umbilicus
2. Posterior abdominal wall:
- T12 – subcostal
- Lumbar (L1-L5): Iliohypogastric and ilioinguinal (L1), Gentitofemoral (L1-L2), Lateral cutaneous femoral (L2-L3), Femoral (L2-L4), Obturator (L2-L4), Lumbosacral trunk (L4-L5)

(II) Nerves of GIT: Visceral – Abdominal viscera and visceral peritoneum
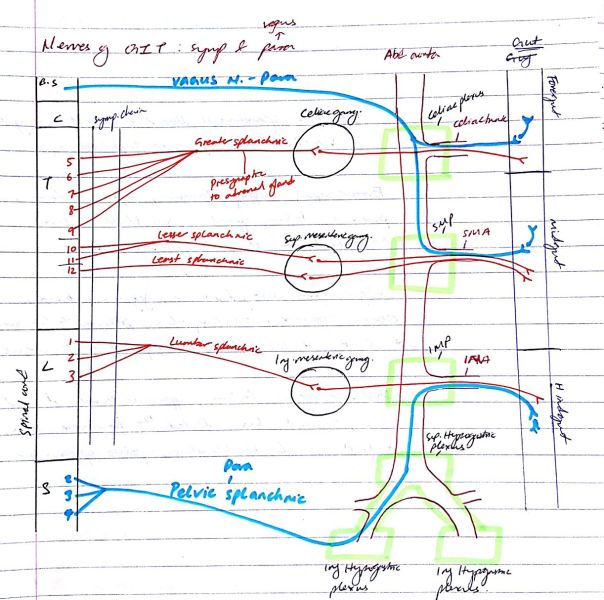
Sympathetic: vasoconstrict blood vessels, decrease peristalsis and digestion, close sphincters of GIT
Parasympathetic: vasodilate blood vessels, increase peristalsis and digestion, stimulate insulin production
NB:
- If a sympathetic nerve is supplying a thoracic viscera – Synapse occurs in sympathetic chain
- If a sympathetic nerve is supplying an abdominal viscera – No synapse, but passes through the chain and synapses at the celiac ganglion, SMG or IMG
1. Presynaptic fibers T5-T9 ⇒ Greater splanchnic nerve – Sympathetic
- Synapse in celiac ganglion
- Post synaptic fibers – pass in celiac plexus – towards branches of celiac trunk and supplies foregut organs
2. Presynaptic fibers T10-T11 ⇒ Lesser splanchnic nerve – Sympathetic
- Synapse in SMG
- Post synaptic fibers – pass in SM plexus – towards branches of SMA and supplies midgut organs
3. Presynaptic fibers T12 ⇒ Least splanchnic nerve – Sympathetic
- Synapse in SMG
- Post synaptic fibers – pass in SM plexus – towards branches of SMA and supplies midgut organs
4. Presynaptic fibers L1-L3 ⇒ Lumbar splanchnic nerve – Sympathetic
- Synapse in IMG
- Post synaptic fibers – pass in IM plexus – towards branches of IMA and supplies hindgut organs
5. Vagus nerve – Parasympathetic
- Presynaptic fibers of vagus – through celiac plexus – synapses at small ganglion of the foregut organ
- Presynaptic fibers of vagus – through SM plexus – synapses at small ganglion of the midgut organ
6. Presynaptic S2,S3,S4 – Pelvic splanchnic nerve – Parasympathetic
- Run in inferior hypogastric plexus – ascend to superior hypogastric plexus – then to inferior mesenteric plexus – along branches of IMA
- Synapse at small ganglion of hindgut organ
Blood and nerve supply of foregut, midgut and hindgut organs
Foregut organs: Esophagus, stomach, 1st part duodenum, pancreas, liver, gallbladder
- Artery – Celiac trunk
- Nerve – Greater splanchnic, vagus
Midgut organs: Rest of duodenum, jejunum, ilium, cecum, appendix, ascending colon, proximal 2/3 transverse colon
- Artery – SMA
- Nerve – Lesser splanchnic, least splanchnic and vagus
Hindgut organs: Rectum, upper anal canal, descending colon, sigmoid colon, distal 1/3 transverse colon
- Artery – IMA
- Nerve – Lumbar splanchnic, pelvic splanchnic
Abdomen
Longitudinal section of abdomen:

Supracolic and infracolic connected by paracolic gutters – drain fluid such as pus or bile to outer margins of colon (Clinical – spread infection, tumor deposits from or to pelvis)

Organs are covered by visceral peritoneum. Between parietal and visceral peritoneum is peritoneal fluid (contains electrolytes, antibodies, WBC, glucose)
Clinical: Ascites – fluid accumulation
Regions of abdomen:
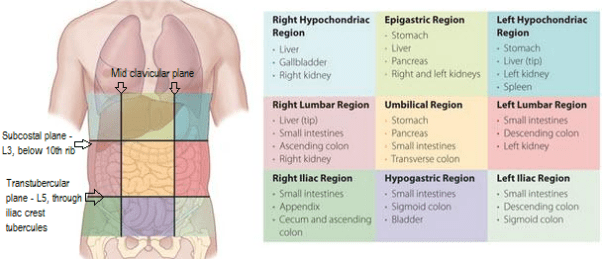
Clinicals:
- Pain location, surgical procedures
- Abdominal hernias:
- Internal – hiatus of diaphragm, epiploic foramen
- External – inguinal, femoral, obturator
Anterior abdominal wall
Layers:
- Skin
- Superficial fascia:
- Above umbilicus – single sheet of connective tissue
- Below umbilicus – fatty Camper’s fascia then membranous Scarpe’s fascia
- Muscles: enclosed in deep investing fascia
- External oblique
- Internal oblique
- Transverse abdominis
- Fascia transversalis
- Extraperitoneal fatty areolar tissue
- Parietal peritoneum
NB:
- In the centre is rectus muscle
- Scarpe’s fascia continues as Colle’s and Darto’s fascia and is inferiorly attached to fascia lata below inguinal ligament. Therefore when penile urethra injured in men, urine escapes urethra to scrotum and spreads in lower abdominal wall but not to thigh.
Functions:
- Contain and protect abdominal contents
- Increase intraabdominal pressure in micturition, defecation, coughing, sneezing and parturition
- Cause trunkal flexion
- Contribute to venous return
Blood supply:
- Internal thoracic – Superior epigastric, musculophrenic
- Abdominal aorta – Posterior intercostal, subcostal
- External iliac – Inferior epigastric, deep circumflex iliac
- Femoral – Superficial circumflex iliac, superficial epigastric
Nerves: Written in nerves
Lymph:
- Superficial:
- Superior to umbilicus – Anterior axillary and parasternal
- Inferior to umbilicus – Superficial inguinal
- Deep: External iliac, lumbar nodes
Anterior Abdominal wall muscles:
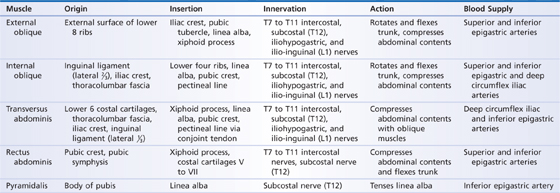
Clinicals:
- Abdominal incision/ Laparotomy – most common is midline incision along linea alba from xiphoid process to umbilicus to pubic symphysis
- Urinary extravasation – penile urethra injured in men, urine escapes urethra to scrotum and spreads in lower abdominal wall but not to thigh
- Venous engorgement – flow in SVC or IVC obstructed, leads to collateral flow
- Ascites
- Caput medusae – engorged superficial epigastric veins
- Liposuction
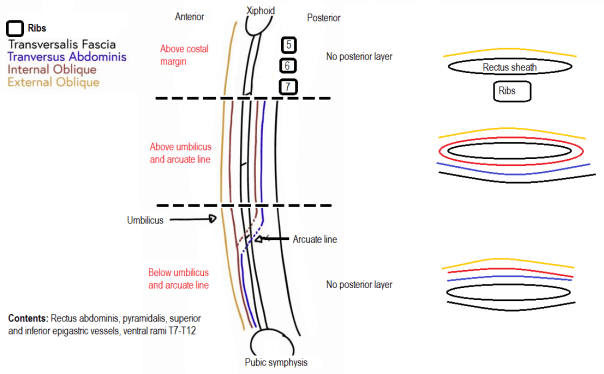
Rectus sheath
Posterior abdominal wall
Fascia:
- Fascia transversalis
- Psoas major fascia
- Thoracolumbar fascia – 3 layers
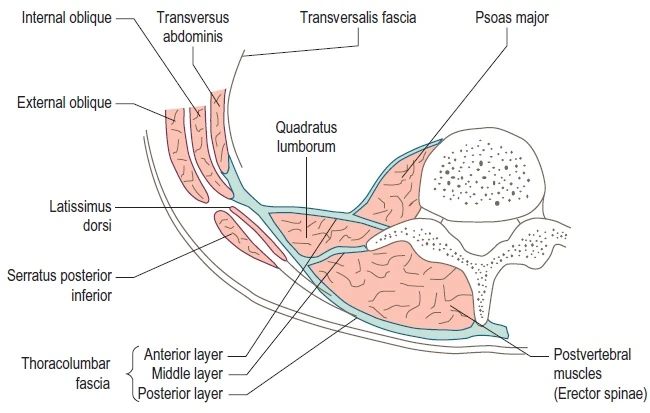
Clinicals:
- Psoas abscess – caused by lumbar tuberculosis, infects psoas sheath
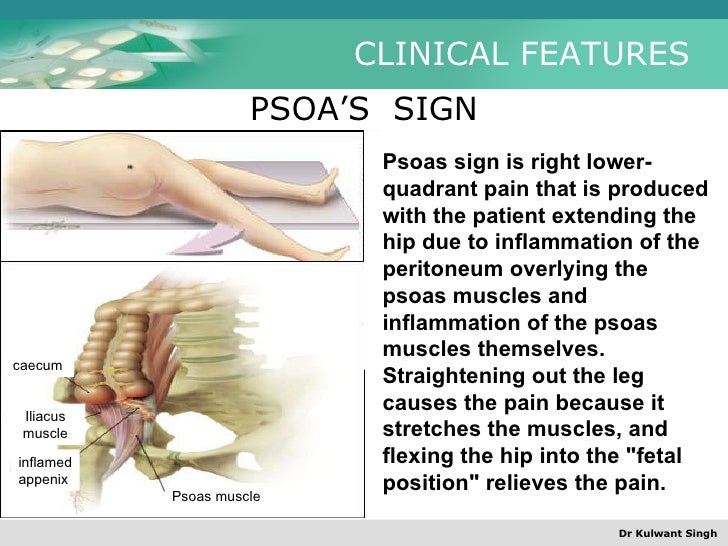
- Psoas sign
Inguinal canal
Superior and parallel to inguinal ligament

Boundaries:
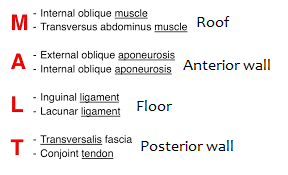
Contents: Ilioinguinal nerve, genitofemoral nerve, round ligament (females), spermatic cord (males)
Inguinal triangle of Hesselbach

Clinicals:

Peritoneum
Closed sac except in females where infundibulum opens
Layers: Parietal and visceral
Intraperitoneal organs: Stomach, spleen, liver, transverse colon
Retroperitoneal organs: Primary (retro since developed – KER) and secondary (become retro later – SADPUC)
Retroperitoneal viscera:
- S – Suprarenal glands
- A – Aorta and IVC
- D – Duodenum (2nd part)
- P – Pancreas
- U – Ureter
- C – Colon (ascending and descending)
- K – Kidney
- E – Esophagus
- R – Rectum
Ligaments:
- Median umbilical ligament (allantoic duct) – urinary bladder apex to umbilicus
- 2 medial umbilical ligaments (umbilical arteries)
- 2 lateral umbilical ligaments – cover inferior epigastric artery
NB: Umbilical vein – becomes ligamentum teres of liver
Mesenteries: Fold of visceral peritoneum that attatches intraperitoneal organs to posterior abdominal wall. Contains nerves, vessels, lymph nodes and fat
Omenta:
- Greater omentum – From greater curvature stomach and proximal duodenum ⇒ to infront of small intestines ⇒ Reflects and ascends to transverse colon

Contains: Nerves, vessels, lymph nodes and fat
Parts: Gastrosplenic ligament, gastrophrenic ligament, gastrocolic ligament
Functions:
- Infection and wound isolation
- Limit spread of intraperitoneal infections
- Immunity – macrophages, lymphocytes etc
- Mobility
- Insulation
2. Lesser omentum – From lesser curvature stomach to liver
Parts: Hepatogastric ligament (right and left gastric arteries), hepatoduodenal ligament (Common bile duct, portal vein, hepatic artery)
Peritoneal cavity:
Epiploic foramen – Relations:
- Superior – Caudate lobe liver
- Inferior – 1st part duodenum
- Anterior – Hepatoduodenal ligament
- Posterior – IVC
Clinicals:
- Internal hernia
- Accumulation of blood (ruptured spleen), bile (bile duct) or fecal matter (intestines)
- Peritonitis – infection due to bacterial contamination
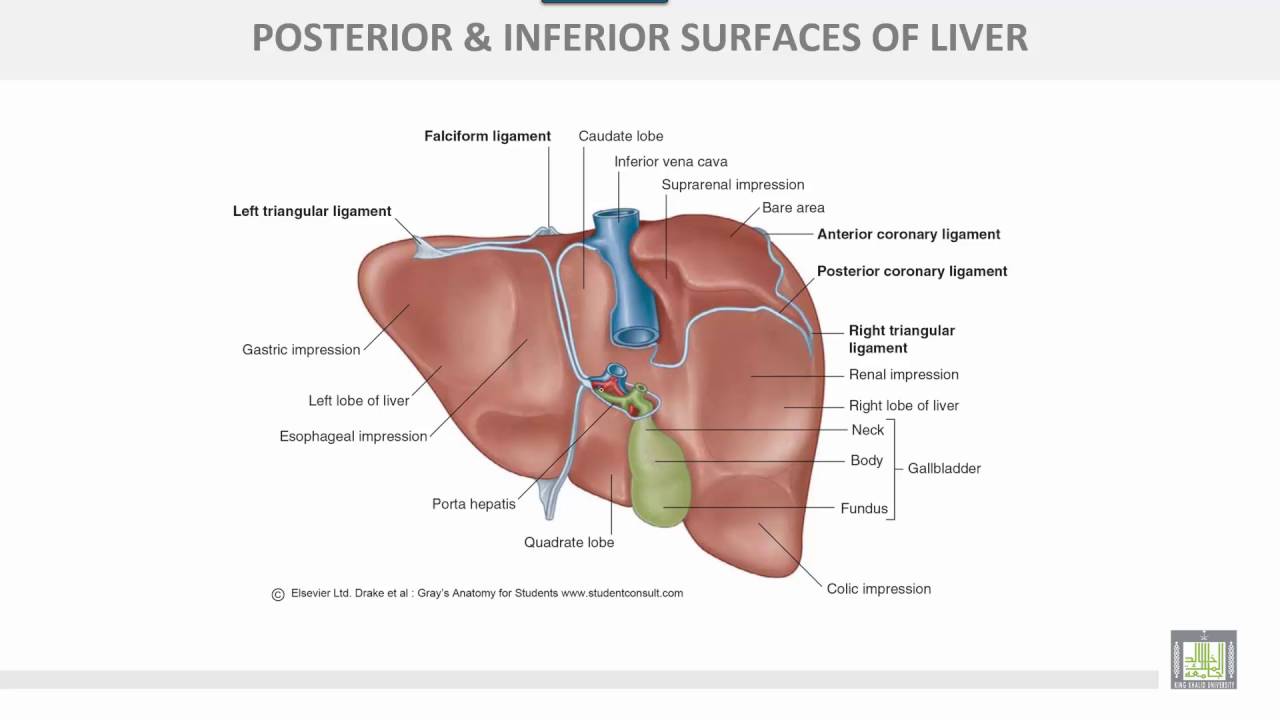
Liver
Ligaments:

Impressions on liver:
Position: Right 1/4, deep to ribs 7-11
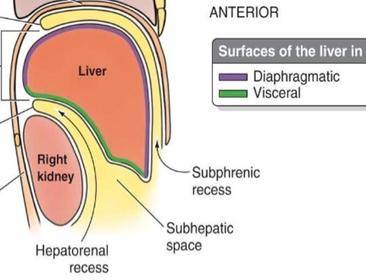
Surfaces: Diaphragmatic and visceral
Relations:
- Anterior: Diaphragm, ribcage, falciform ligament
- Posterior: Right kidney and adrenal, gall bladder, esophagus, stomach
- Superior: Diaphragm
- Inferior: Gall bladder
Support structures: Falciform ligament, coronary ligament, ligamentum teres, triangular ligament, hepatoduodenal ligament, lesser omentum and hepatic veins
Blood supply: Right and left hepatic arteries – segmental branches
Venous: Hepatic portal vein – drains to hepatic sinusoids and so to IVC
Nerves: Sympathetic – Greater splanchnic, Parasympathetic – Vagus, right phrenic
Lymphatics: Hepatic, left gastric nodes
Hepatic recesses:
- Right and left subphrenic spaces – between diaphragm and liver
- Subhepatic space – between inferior surface liver and transverse colon
- Morrison’s pouch/ hepatorenal – between liver and right kidney
Functional divisions of liver:
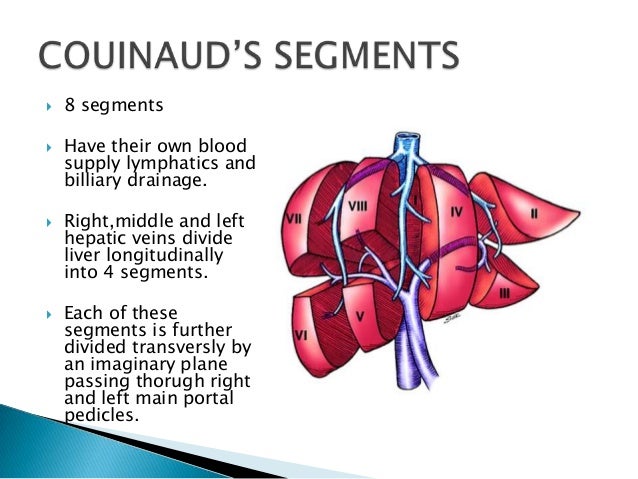
Clinicals:
- Hepatic lobectomies
- Rupture of liver – fractured rib, hemorrhage
- Liver trauma – tearing of hepatic veins from IVC
- Hepatomegaly – enlarged liver – due to infection, tumours or metabolic disorder
- Liver cirrhosis – health tissue replaced by scar tissue, organ will start to fail, blood cannot easily flow in portal vein
- Liver biopsy – small needle inserted in liver to collect tissue sample
- Jaundice
Gallbladder
Location: Between right and left lobes, inferior surface of liver
Biliary tree:

Relations:
- Anterior – Inferior surface liver
- Posterior – Transverse colon, proximal duodenum
- Superior – Liver
- Inferior – Biliary tree
Blood: Cystic artery
Venous: Cystic vein, hepatic sinusoids
Nerves: Sympathetic – Greater splanchnic, Parasympathetic – Vagus, right phrenic
Lymph: Hepatic nodes
Clinicals:
- Mobile gallbladder – only attached to cystic duct, risk of torsion
- Cholecystectomy
- Gall stones
- Biliary colic – gall stones block bile duct
- Cholecystitis – inflammation
Spleen
Impressions:

Surfaces: Diaphragmatic and visceral
Relations:
- Anterior: Stomach
- Posterior: Left kidney and adrenal, ribs 9-11
- Inferior: Left colic flexure
Support structures:
- Gastrosplenic ligament (short gastric vessels) – great curvature to spleen
- Splenorenal ligament (Splenic vessels) – spleen to left kidney
- Phrenicocolic ligament – diaphragm to left colic flexure
Blood supply: Splenic artery – 5 segmental arteries
Venous: Splenic vein
Nerves: Sympathetic – Greater splanchnic, Parasympathetic – Vagus, right phrenic
Lymphatics: Celiac nodes
Clinicals:
- Rupture of spleen – fractured rib, intraperitoneal hemorrhage
- Splenectomy
- Splenomegaly
- Accessory spleen
- Splenic biopsy
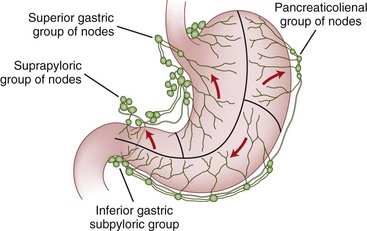
Stomach

Relations:
- Anterior – Left lobe liver
- Posterior – Lesser sac, spleen, left kidney and adrenal, splenic artery, pancreas, aorta
- Inferior – Transverse colon, left colic flexure
Blood supply:

Nerves: Sympathetic – Greater splanchnic, Parasympathetic – Vagus, right phrenic
Lymphatics:
Clinicals:
- Esophageal varices – portal hypertension
- Pyrosis (heart burn) – due to gastroesophageal reflex disorder (stomach acid flows to esophagus)
- Gastroesophageal reflex disorder – hiatus hernia, delayed gastric emptying, dysfunction of lower esophagus sphincter
- Hiatus hernia – part of stomach protrudes through esophageal hiatus in diaphragm
- Pylorospasm – closure of pylorus due to muscle spasm, due to pyloric ulcers
- Gastrectomy
- Gastric ulcers – erode arteries nearby
Pancreas
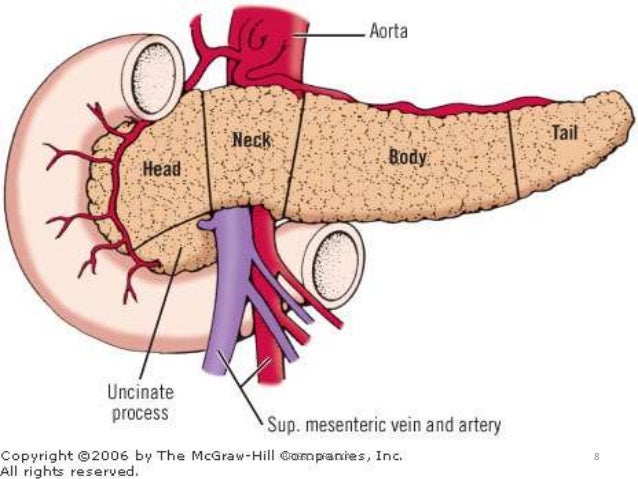
Relations:
Blood supply: Greater pancreatic artery (from splenic artery), Superior and inferior pancreaticoduodenal artery
Nerves: Sympathetic – Greater splanchnic, Parasympathetic – Vagus, right phrenic
Lymphatics: Pancreaticosplenic, pancreaticoduodenal
Clinicals:
- Blocked hepatopancreatic ampulla – gallstone
- Pancreatitis
- Pancreatic ectomy
- Rupture
- Cancer
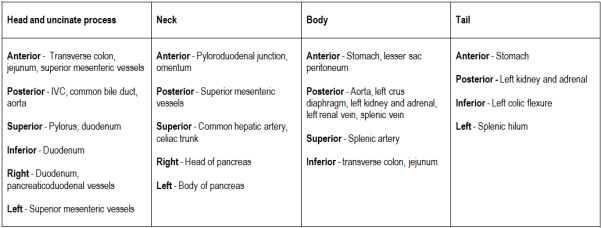
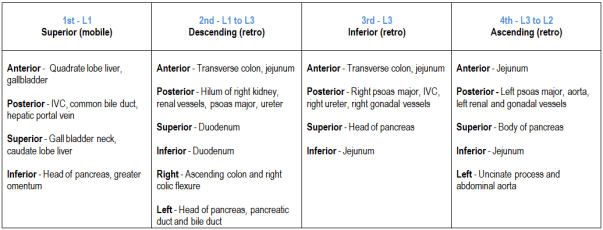
Duodenum
From pylorus to duodenojejunal junction

Relations:
Support structures: Hepatoduodenal ligament, ligament of Trietz
Recesses:

Blood supply: Superior and inferior pancreaticoduodenal, right gastroepiploic
Nerve: Sympathetic – Greater and lesser splanchnic, Parasympathetic – Vagus
Lymphatics: Pancreaticoduodenal nodes, superior mesenteric nodes
Clinicals:
- Duodenal ulcers – erode gastroduodenal artery – hemorrhage
- Paraduodenal hernia – intestinal loops
Jejunum and ileum
From duodenojejunal junction to ileocecal junction

Blood supply: SMA and vasa recta
Nerves: Lesser splanchnic, least splanchnic and vagus
Clinicals: Ischemia of intestine – occlusion of vasa recta by embolus
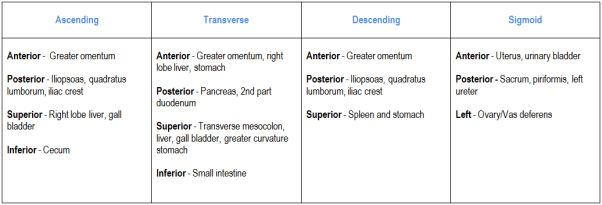
Large intestine
From ileocecal valve in right iliac fossa to anal orifice

NB: Ascending colon has no mesentary
Relations:
Blood supply:

Nerves:
- Lesser splanchnic, least splanchnic and vagus – Cecum, appendix, ascending colon, proximal 2/3 transverse colon
- Lumbar splanchnic and pelvic splanchnic – Distal 1/3 transverse, descending and sigmoid coloc
Lymphatics: Epicolic and paracolicdrain into superior and inferior mesenteric nodes
Clinicals:
- Colitis
- Colectomy
- Ileostomy – artificial opening of ileum through abdominal wall
- Colonoscopy
- Diverticula – pouches form on wall of colon (usually sigmoid) – old people
- Volvulus sigmoid- sigmoid colon twists on sigmoid mesocolon – bowel obstruction
Difference between small and large intestine:

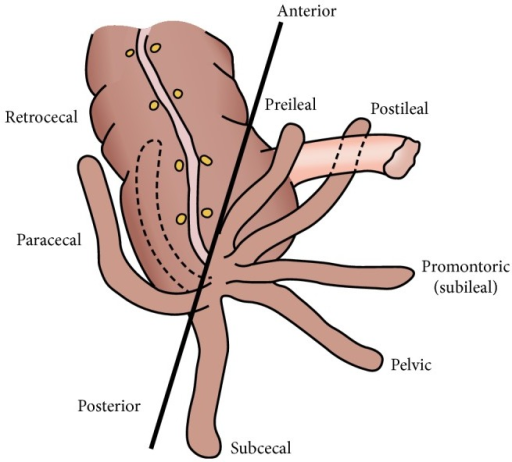
Appendix
Location: Right iliac fossa, opens in cecum
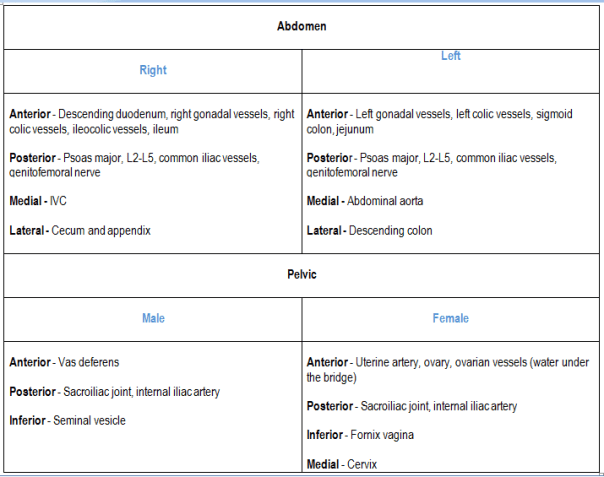
Relations:
- Anterior – Greater omentum
- Posterior – Psoas major
- Superior – Ileum, mesoappendix (portion of the mesentery connecting the ileum to the appendix)
- Left – Sigmoid colon
- Right – Paracolic gutter, ascending colon
Positions:
Blood supply: Appendicular artery and vein
Nerves: Lesser splanchnic, least splanchnic and vagus
Lymphatics: Superior mesenteric
Clinicals:
- Appendicitis
- Appendectomy
- Psoas test
Kidneys
Are 3 vertebrae long
Coverings: Superficial to deep
Pararenal fat ⇒ Renal fascia (enclose kidney and suprarenal glands) ⇒ Perirenal fat ⇒ Fibrous renal capsule
Support structures: Splenorenal ligament
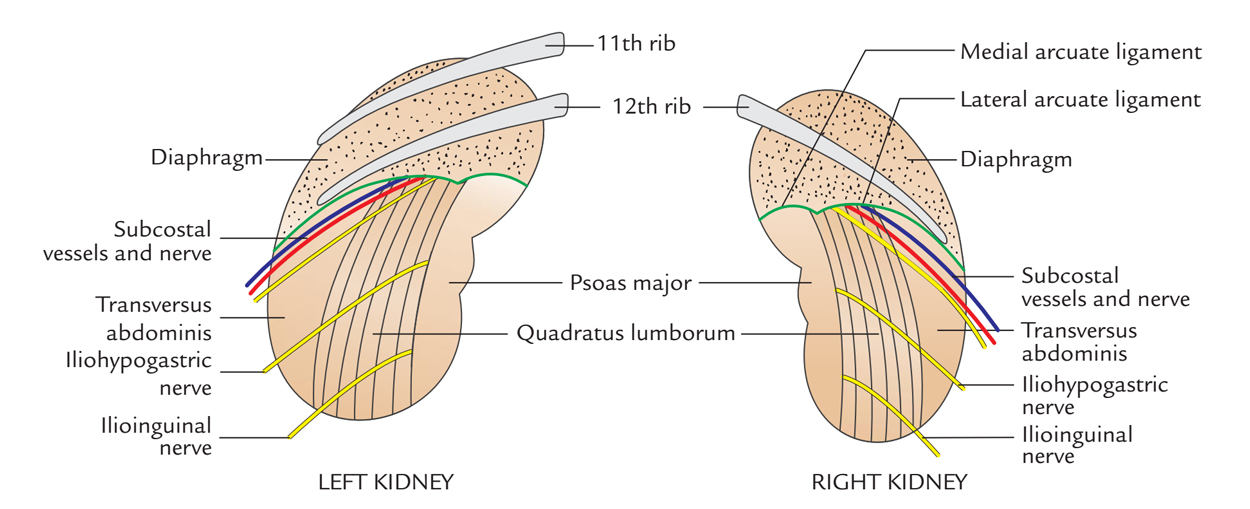
Relations:
Anterior:
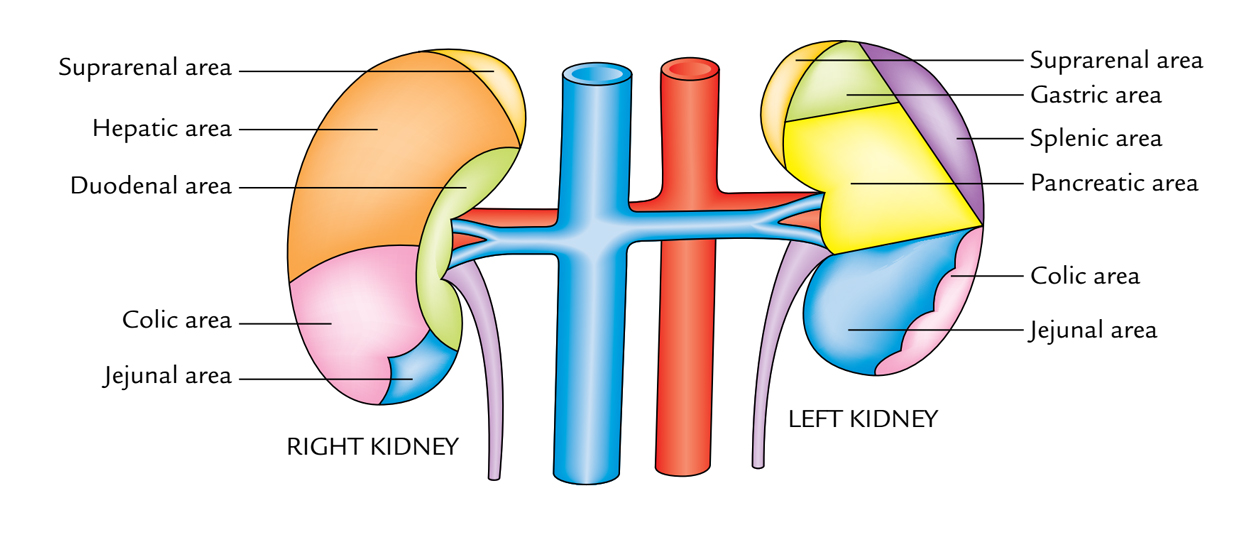
Posterior:
Blood supply:

Nerves: Lesser splanchnic, least splanchnic and vagus
Lymphatics: Lumbar nodes
Clinicals:
- Perinephric abscess – pus around kidney
- Pelvic kidney
- Horseshoe kidney
- Renal agenesis
- Renal hypoplasia
- Kidney stones/renal calculi – formed in kidney or renal pelvis, may pass through ureter into bladder
- Renal transplant – to lower abdomen, renal vessels connected to recipient external iliac vessels, ureter sutured into urinary bladder
- Nephrectomy
- Floating kidney – abnormal condition in which the kidney drops down into the pelvis when the patient stands up
Suprarenal glands
Cortex (mesoderm) and medulla (ectoderm – neural crest). Fatty tissue between kidney and suprarenal gland, covered in renal fascia.
Relations:
Right:
- Anterior – Right lobe liver
- Posterior – Right crus diaphragm
- Superior – Liver
Left:
- Anterior – Stomach, pancreas, spleen
- Posterior – Left crus diaphragm
- Superior – Spleen
Blood supply: Superior, middle and inferior suprarenal
Venous: Right and left suprarenal
Nerves: Greater splanchnic, lesser splanchnic
Lymphatics: Lumbar nodes
Right and left difference:
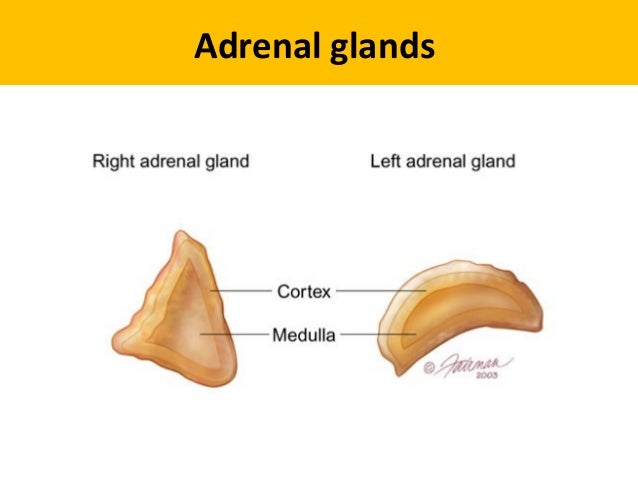
Right – Triangular shape, loosely attached to superior pole kidney
Left – Cresent shape, superior and middle border can extend to renal hilum
Clinicals:
- Tumor of medulla
- Addison’s disease – low cortisol and aldosterone
- Cushing’s syndrome – elevated cortisol
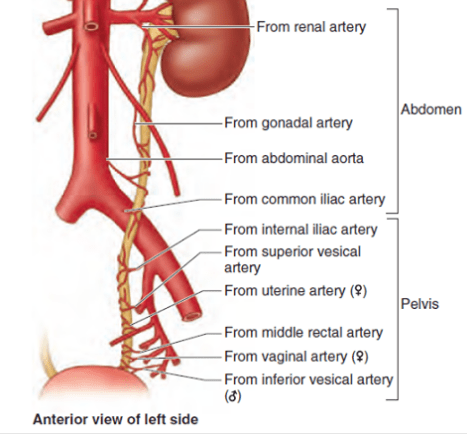
Ureter
Course:
- Continuation of renal pelvis
- Posterior to renal vessels
- Anterior to psoas major
- Gonadal vessels cross over it from medial to lateral
- Cross infront of common iliac bifurcation
- Opposite sacroiliac joint
- Opposite ischial spine, curves anteromedial to open into posterior superior part of bladder
- Runs an oblique 2cm course in urinary bladder wall – forms valve like mechanism
Blood supply:
Nerves: Renal plexus, superior hypogastric plexus, T11-L2
Lymphatics: Lumbar, common iliac, external iliac, internal iliac
Relations:
Clinicals:
- Retrocanal ureter – Right ureter passes posterior to IVC, disturbs drainage from right kidney
- Kidney stones – Obstruct urine flow
Others
1. Lumbar triangle:

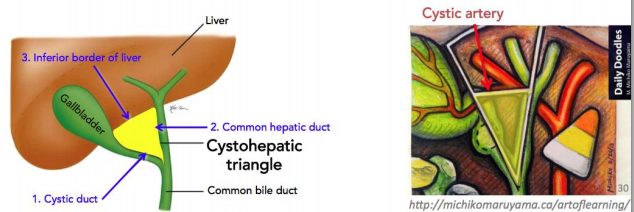
2. Calot’s triangle/Cystohepatic triangle:
Content: Cystic artery
3. Triangle of doom:
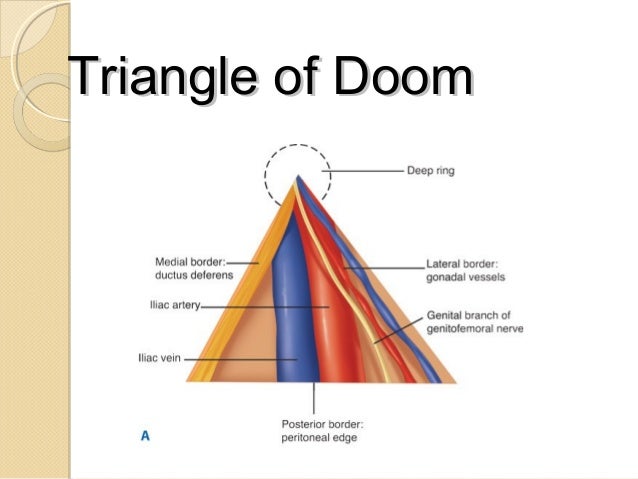
Contents:
- External iliac vessels
- Deep circumflex iliac vein
- Femoral nerve
- Genital branch of genitofemoral nerve
Clinicals: Inguinal hernia – nerves damaged when repairing a hernia by sutures or staples
4. Triangle of pain:

5. Triangle of safety:
For intercostal catheter placement

6. Modification of fascia transversalis:
- Femoral sheath and ring – anterior
- Deep inguinal ring – posterior
- Internal spermatic fascia in testis
7. Mcburney’s point:

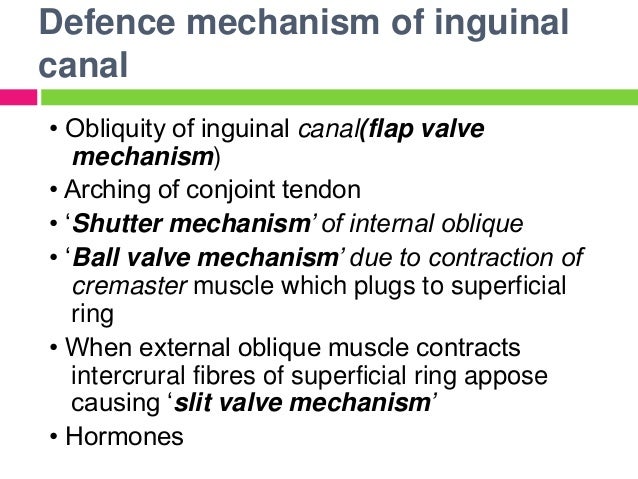
8. Mechanisms to prevent inguinal hernia:
These are summarized notes from various sources, mainly TeachMeAnatomy and Wikipedia
