Development of kidney, urinary bladder and urethra
Kidney
Intermediate mesoderm: kidneys, ureters and trigone of urinary bladder
Endoderm: rest of urinary bladder, urethra
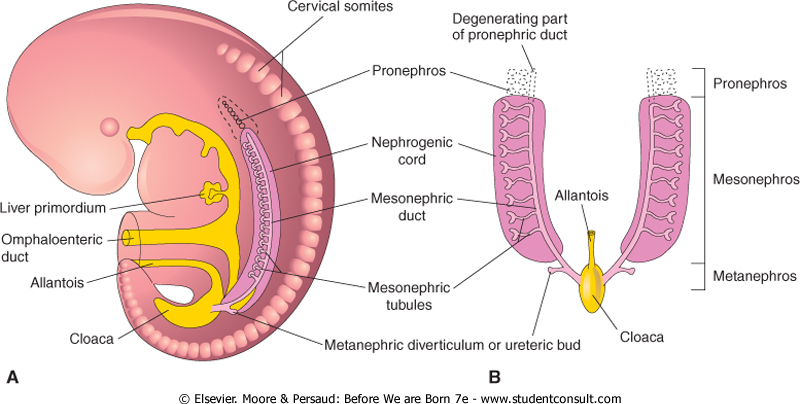
3 kidneys develop: Pronephros, mesonephros and metanephros
(I) Pronephros:
Segmented cervical intermediate mesoderm
7-10 excretory tubules called pronephric tubules form – degenarate by end of 4th week
Collecting duct called pronephric duct forms and opens down into cloaca – pronephric duct persists to form mesonephric duct
(II) Mesonephros:
Segments of thoracic and upper lumbar region of intermediate mesoderm
Each segment forms 2-3 ‘S’ shaped mesonephric tubules
Lateral ends open in mesonephric duct and medial end invaginated by glomerulus
In males:
Mesonephric tubules: upper degenerate, rest form efferent ducts of testis, head of epididymis, paradidymis
Mesonephric duct: body and tail of epididymis, vas deferens, ejaculatory duct, seminal vesicle, ureteric bud and trigone of urinary bladder
In females:
Mesonephric tubules: degenerate
Mesonephric duct: ureteric bud and trigone of urinary bladder
(III) Metanephros: (kidneys)
(A) Development of collecting duct and ureter:
Ureteric bud develops from mesonephric duct
Ureteric bud grows cranially, and penetrates metanephric cap
Upper end of ureteric bud enlarges ⇒ forms pelvis which divides into ⇒ 2-3 major calyces ⇒ where each divides into minor calyces ⇒ then collecting tubules ⇒ which join to nephrons
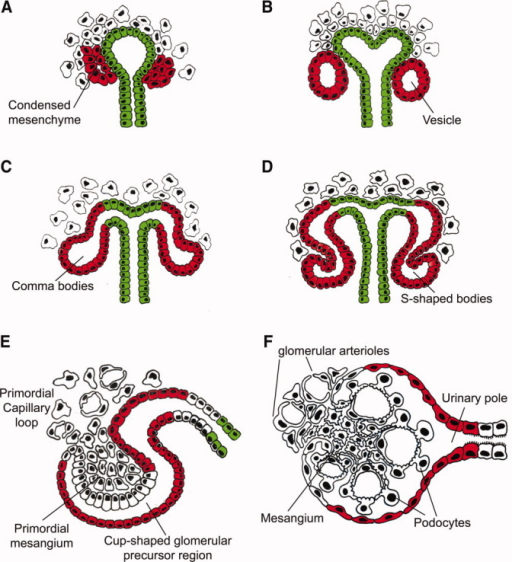
(B) Development of nephrons:
Caudal part of intermediate mesoderm forms a metanephric cap
Which divides into renal vesicles
Each renal vesicle surrounds the free end of a collecting tubule and forms a ‘S’ shaped nephron
One end of nephron invaginated by glomerulus – Bowman’s capsule
Other end joins collecting duct
Each nephron elongates – forms proximal and distal convolutes tubules and loop of Henle
Further growth of kidney:
Lobulated grooves disappear – forms smooth surface
Ascends from pelvic region to adult level
Recieves blood supply from median sacral, common iliac, lower abdominal aorta. Then only from aorta
At first, hilum directed forwards, rotates 90 degrees so hilum becomes medial
Congenital anomalies of kidney:
Renal agenesis
Renal hypogenesis – small size
Congenital polycystic kidney – failure of fusion between nephrons and collecting tubules. Urine collects in nephrons, dilates and forms cysts, nephrons destroyed
Pelvic kidney – failure of ascent
Horseshoe shaped kidney – fusion of both kidneys, ureters kinked, this causes urinary stasis and so infection
Additional branches of aorta supplying kidney – cross infront of ureter and compress it – urinary stasis
Double ureter – 2 ureteric buds/ early splitting of ureteric bud. More liable to infection and stone formation
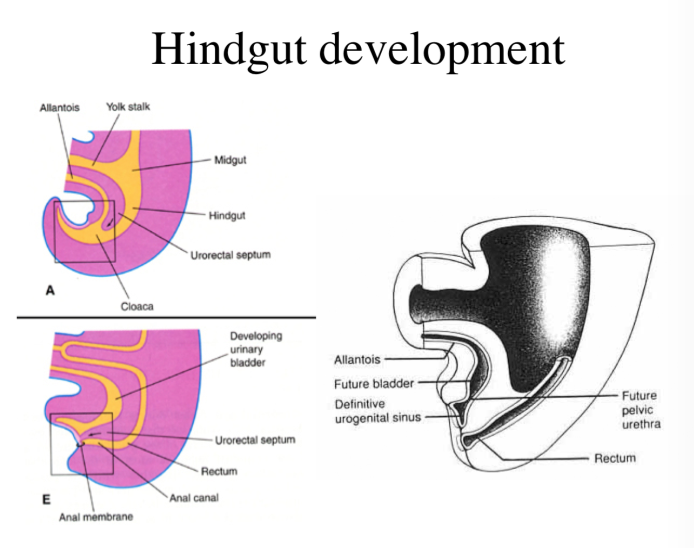
Urinary bladder and urethra
A constriction appears in primitive urogenital sinusat site of entrance of mesonephric duct
Divides into:
Upper part – Vesico-urethral canal
Lower part – Definitive urogenital sinus
(I) In males
(A) Urinary bladder:
From vesico-urethral canal
Trigone from absorbed common stem of mesonephric duct and ureter.
Differential growth of posterior bladder wall, therefore ureter moves upwards (posterior superior angle)
(B) Seminal vesicle:
Develops as a diverticulum from vas deferens. Part distal to it becomes ejaculatory duct.
3. Penile urethra – Definitive urogenital sinus forms a urethral plate that extends on the under surface of phallus (primitive penis) and is surrounded by 2 urethral folds – unite from back and front around urethral plate to form penile urethra. Lined by endoderm, terminal glandular part lined by ectoderm.
(D) Prostate gland:
Develops from 15 to 20 buds from prostatic urethra
Canalized to form alveoli and ducts
Connective tissue and capsule from surrounding mesoderm
(II) In females
Vesicourethral canal – urinary bladder and urethra
Definitive urogenital sinus – lower 1/5 vagina and vestibule
Congenital anomalies:
Urachal fistula – unobliterated urachus. Urine drips from umbilicus
Urachal cyst – Incomplete obliteration
Bladder extrophy – urinary bladder opens into anterior abdominal wall
Hypospadius – external urethral meatus opens on under surface of penis
Epispadius – external urethral meatus opens on upper surface of penis
It is a thick mass of mesoderm which partially separates thoracic cavity and abdominal cavity.
Forms in neck by fusion of 3, 4, 5 cervical myotomes
Motor nerve is phrenic nerve
Embryonic disc folds and heart descends, therefore septum transversum is pushed caudally and pulls the phrenic nerve with it
Derivatives:
Superior layer – formation of fibrous pericardium
middle layer – diaphragm muscle, central tendon, diaphragmatic pleura and peritoneum
Inferior layer – fibrous capsule and connective tissue of liver, ventral mesentery of the gut
Diaphragm
Origin: Mesoderm
Diaphragm develops from:
Septum transversum – Central tendon, sternal and costal parts of diaphragm
2 pleuro-peritoneal membranes – 2 mesodermal folds that project inwards from body wall. Close pleuro-peritoneal canals. Forms dorsilateral part of diaphragm
Mesoderm from chest wall – marginal part of diaphragm
Mesentery of esophagus – Posterior medial part and crura of diaphragm
Mesoderm around aorta – lumbar part of diaphragm
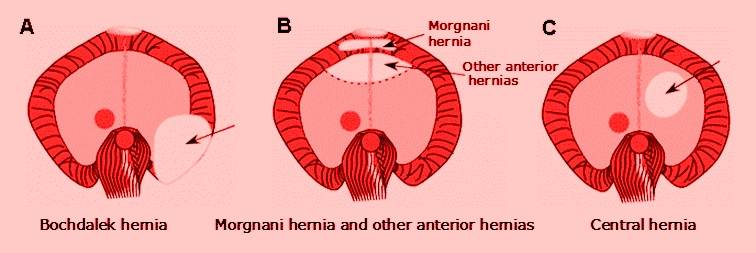
Congenital anomalies:
Parasternal hernia of Morgagni – failure to develop a small part of diaphragm between sternal and costal part
Esophageal hernia – Protrusion of stomach in thorax
Congenital diaphragmatic hernia of Bochdalek – failure of pleuro-peritoneal membranes to close the pleuro-peritoneal canals. Abdominal vicera enter pleural cavity, compress heart and lungs
Second layer of cells develop from coelomic mesothelium and surrounds fetal cortex to form permanent cortex
Fetal cortex regresses and disappears after 3rd year of birth
Permanent cortex differentiates into 3 zones: zona glomerulosa, zona fasiculata and zona reticularis. Complete histological differentiation attained at puberty.
Congenital anomalies:
Agenesis
Ectopic suprarenal gland – below capsule of kidney
Accessory cortical tissue – found on posterior abdominal wall and pelvis
Adrenogenital syndrome – hypertrophy of suprarenal cortex and over production of androgens. Results of pseudohermaphroditism in females and premature enlargement of external genitalia in males
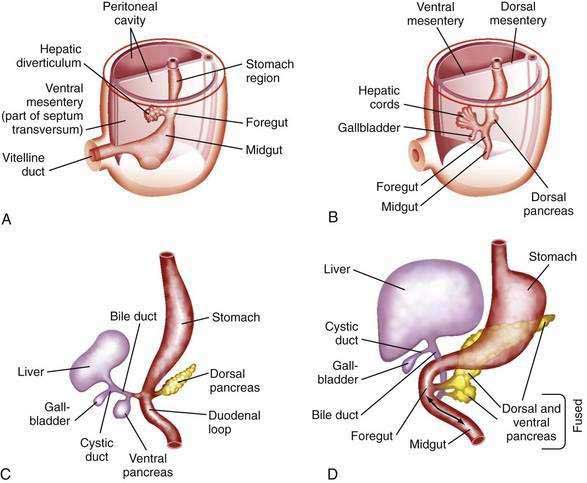
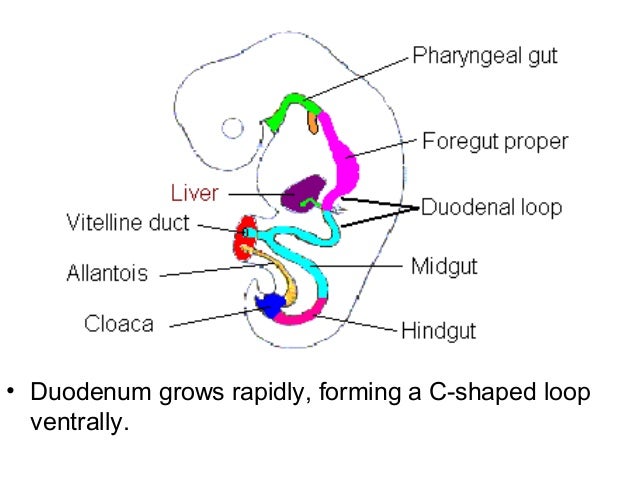
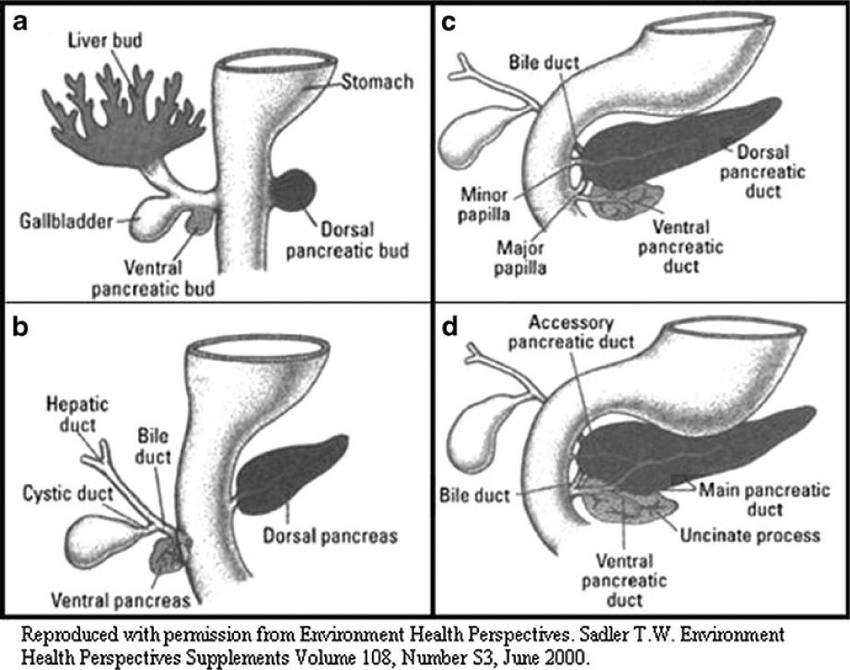
Pars hepatica invades septum transversum and divides into right and left branches (right and left hepatic ducts) which branch more to form columns of hepatic cells
Columns of hepatic cells meet vitelline veins and break them into hepatic sinusoids
Mesoderm of septum transversum forms fibrous tissue stroma and capsule of liver
Original stalk of liver bud elongates – forms common bile duct
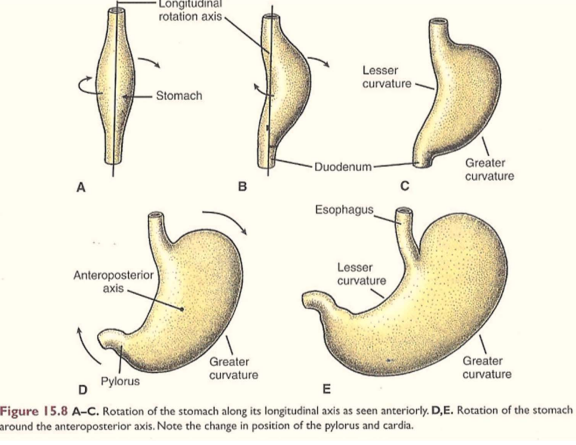
Due to rotation of stomach, common bile duct opens in posterior medial part of 2nd duodenum
Ligaments of liver:
Mesoderm of septum transversum between liver and anterior abdominal wall forms falciform ligament. Umbilical vein lies on inferior free margin of falciform ligament
Mesoderm of septum transversum between liver and stomach forms lesser omentum
Liver separates from septum transversum except “bare area” of liver
Rest of septum transversum forms part of diaphragm