Scalp
Extents:
- Superior nuchal line – posteriorly
- Supraorbital margins – anteriorly
- Zygomatic arch – lateral
Layers:

NB: Injury to scalp leads to prolonged bleeding due to rich blood supply and separation of vessel ends by connective tissue and aponeurosis. Also heals rapidly due to rich blood supply.
Nerves and arteries:

Venous:
- Supraorbital and supratrochlear drain into – facial vein
- Superficial temporal veins – retromandibular vein
- Posterior auricular veins – external jugular veins
- Occipital vein – vertebral veins
NB: The veins connect with intracranial sinuses through emissary veins (can spread infection)
Cranial meninges
3 layers of connective tissues that:
- Protect brain
- Provide framework for arteries and veins
- Enclose fluid filled cavity

(I) Dura mater:
Made of 2 layers that separate to form sinuses:
- Outer periosteal layer
- Inner meningeal layer
(II) Arachnoid mater:
- Avascular layer
- Attached to pia mater by web like arachnoid trabeculae
- Held against dura by pressure of CSF (cerebrospinal fluid)
(III) Subarachnoid space:
Contains arachnoid trabeculae, CSF, blood vessels and nerves
(IV) Pia mater:
- Vascularised
- Thin membrane that adheres to brain surface and follows its contours
- Prevents blood vessels coming in contact with neural tissue
Arterial supply to meninges:
- Middle meningeal artery
- Accessory meningeal artery
- 2 anterior meningeal arteries
- 2 posterior meningeal arteries
Clinicals:
- Epidural hemorrhage – injury to middle meningeal artery
- Subdural hemorrhage – superior saggital veins tear as they drain into superior saggital sinus
- Cerebral hemorrhage – middle cerebral artery branch ruptures
- Meningitis
Dural folds
Invagination of meningeal layer of dura mater – to compartmentalize and stabilize brain
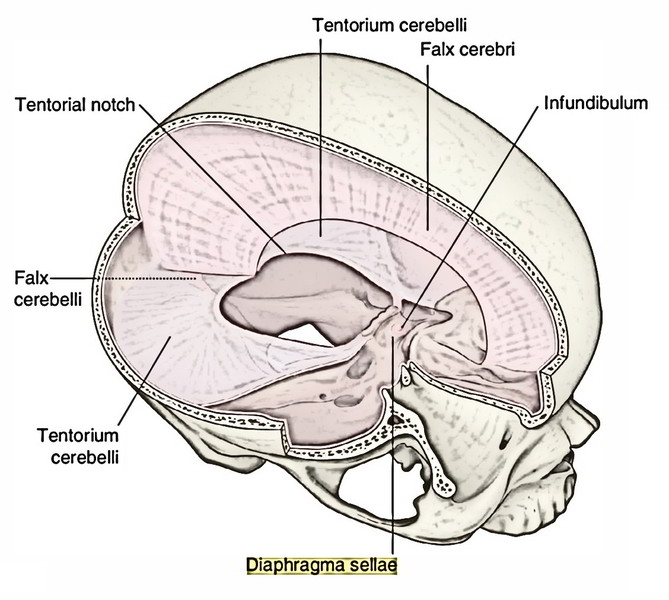

- Falx cerebri – Separate right and left cerebrum
- Falx cerebelli – Separate right and left cerebellum
- Tentorium cerebelli – Separates cerebellum and occipital lobes of cerebrum
- Diaphragm sellae – Roof of sella turica
Dural sinuses
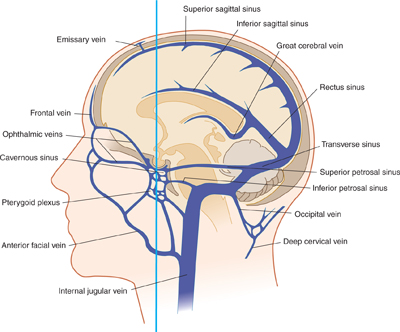
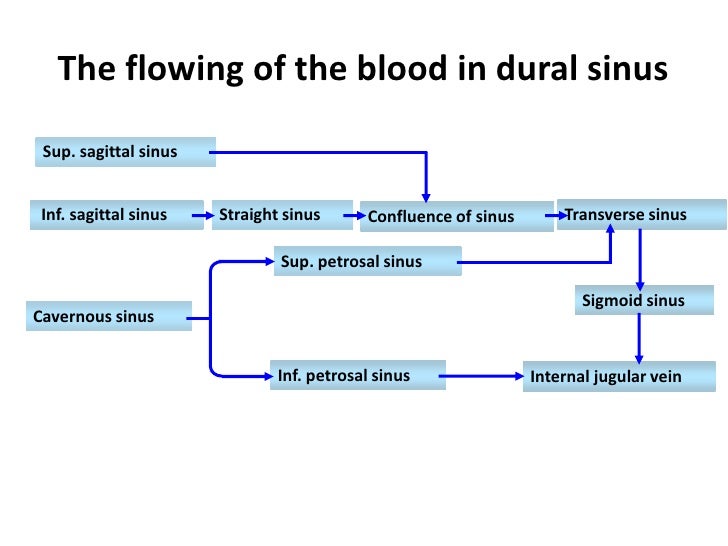
NB: Great cerebral vein joins inferior sagittal sinus to form straight sinus
Blood from superior sagittal sinus favours right transverse sinus
The skull
3 components:
- Neurocranium/ calvaria
- Chondrocranium/ skull base
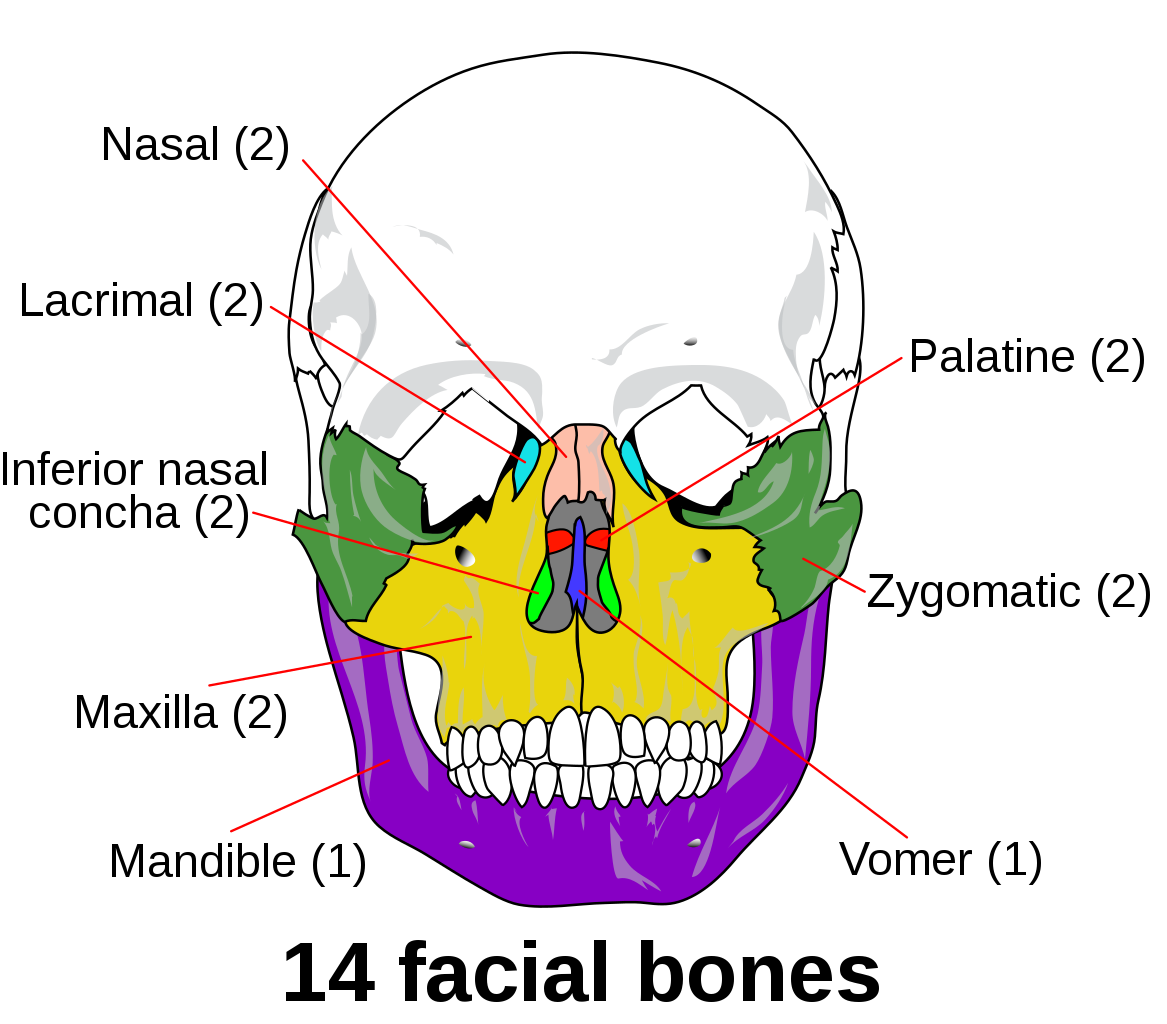
- Vicerocranium/ facial skeleton
Neurocranium:

Chondrocranium:

Vicerocranium:
Sutures of skull

Difference between adult and neonate skull:
1. Ratio of vicerocranium : neurocranium
- Neonate 1:8
- Adult 3:8
2. In neonate, has fontanelles which close:
- Posterior – 3 months after birth
- Sphenoid – 6 months
- Mastoid – 18 months
- Anterior – 18-24 months
3. Neonate does not have all air sinuses
4. Neonate has less prominent mastoid
5. Neonate angle of mandible more obtuse
6. Neonate has no alveolar process
7. Neonate has no styloid process
8. Neonate basal skull ossifies after birth
9. Neonate has no diploe – to enable bone molding during birth
10. Neonate has metopic/frontal suture which disappears after 2 years
Functions of sutures:
- Allow for birth
- Molding and brain growth
- Age estimation
- Draw CSF and blood from fontanelles
Clinicals:
1. Pterion – Thin and weak, made of Frontal, parietal, squamous temporal and greater wing sphenoid. Overlies middle meningeal artery (anterior division). Therefore fracture can damage the artery and lead to epidural hematoma
2. Raised intracranial pressure – bulges anterior fontanelle
3. Sunk anterior fontanelle – dehydration due to diarrhea and vomit
4. Hydrocephaly: Accumulation of CSF, widening spaces called ventricles
- Communicating – CSF no reabsorbed but can flow from ventricle to ventricle
- Non communicating – Obstruction in flowing from one ventricle to another

Cranial fossa
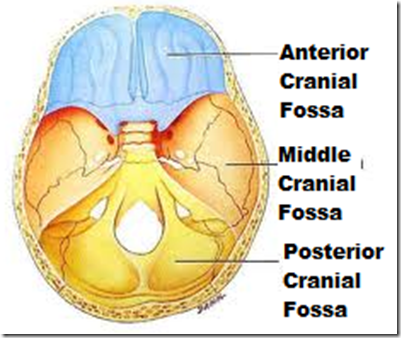
(I) Anterior cranial fossa
Borders:
- Anterior – Frontal bone
- Posterior – Lesser wing sphenoid
- Medial – Cribriform plate
- Lateral – Orbital of frontal bone
- Floor – All of the above
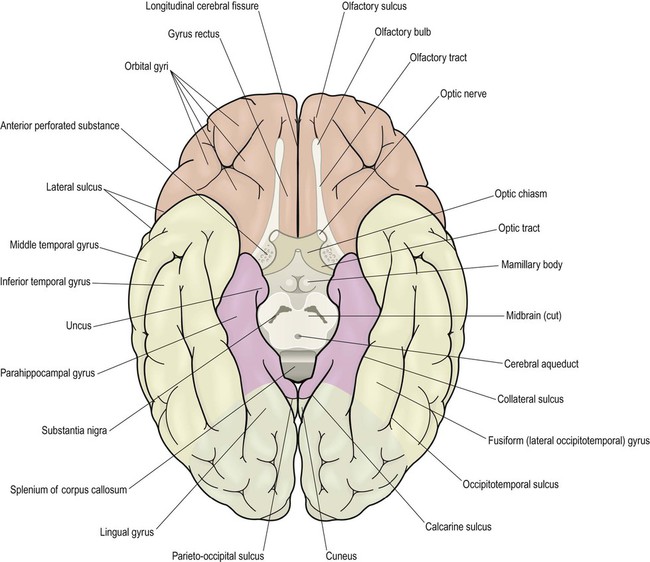
Contents: Frontal lobe, olfactory bulb and tract
Clinicals: Cribriform fracture: loss of smell, CSF in nasal
(II) Middle cranial fossa
Borders:
- Anterior – Lesser wing sphenoid
- Posterior – Petrous temporal
- Medial – Greater wing shenoid
- Lateral – Squamous temporal and parietal bone
- Floor – Sella turcica and greater wing sphenoid
Contents: Temporal lobes, cavernous sinus, pituitary gland, optic chiasma
Clinicals: Pituitary surgery
(III) Posterior cranial fossa
Borders:
- Anterior – Dorsum sellae, petrous temporal
- Posterior – Squamous occipital
- Medial – Dorsum sellae
- Lateral – Mastoid temporal
- Floor – Tentorium cerebelli and occipital bone
Contents: Cerebellum, pons, medulla
Clinicals: Cerebellum tonsillar herniation via foramen magnum
Skull foramina and contents
1. Foramen cecum: Emissary veins (nasal to superior sagittal sinus)
2. Cribriform foramina: Olfactory nerve (CN 1) – nasal to olfactory bulb
3. Optic canal:
- Optic nerve (CN 2) – surrounded with meninges
- Opthalmic artery branch – lacrimal artery
4. Superior orbital fissure:
- Oculomotor nerve (CN 3)
- Trochlear nerve (CN 4)
- Abducens nerve (CN 6)
- Opthalmic nerve (CN 5-1)
- Superior opthalmic vein
5. Foramen rotundum: Maxillary nerve (CN 5-2)
6. Foramen ovale: MALE
- Mandibular nerve (CN 5-3)
- Accessory meningeal artery
- Lesser petrosal nerve
- Emissary veins (pterygoid plexus – cavernous sinus)
7. Foramen lacerum:
- Greater petrosal nerve
- Internal carotid artery
8. Foramen spinosum:
- Middle meningeal artery
- Middle meningeal vein
- Nervous spinosus (nerve branch of 5-3)
9. Carotid canal: Internal carotid artery
10. Internal acoustic meatus:
- Facial nerve (CN 7)
- Vestibulocochlear nerve (CN 8)
- Labyrinthine artery
11. Jugular foramen:
- Glossopharyngeal nerve (CN 9)
- Vagus nerve (CN 10)
- Accessory nerve (CN 11)
- Inferior petrosal sinus
- Sigmoid sinus
- Posterior meningeal artery
12. Mastoid foramen:
- Facial nerve (CN 7)
- Emissary veins
13. Hypoglossal canal: Hypoglossal nerve (CN 12)
14. Foramen magnum:
- Medulla
- Meninges
- Vertebral arteries
- Spinal arteries

15. Supraorbital foramen: Supraorbital nerve (from frontal nerve from opthalmic nerve 5-1)
16. Infraorbital foramen: Infraorbital nerve of 5-2
17. Mental foramen: Mental nerve
Cranial nerves
- Olfactory – Sensory
- Optic – Sensory
- Oculomotor – Motor
- Trochlear – Motor
- Trigeminal – Both
- Abducens – Motor
- Facial – Both
- Vestibulocochlear – Sensory
- Glossopharyngeal – Both
- Vagus – Both
- Accessory – Motor
- Hypoglossal – Motor
Mnemonic: Oh Oh Oh To Touch And Feel Very Good Velvet Ah Heaven!
Mnemonic: Some Say Marry Money But My Brother Says Big Brains Matter Most
Cranial nerve courses
NB: Summarised notes made from: Teachmeanatomy
(I) Olfactory nerve: Special Viceral Afferent (smell)
- Olfactory mucosa containing non myelinated axons
- Axons bundle to form a bundle – filia olfactoria
- Pass through cribriform plate foramina
- Enter olfactory bulb
- Olfactory nerves synapse with mitral cells
- Forming a synaptic glomeruli
- The mitral cells run posteriorly in the olfactory tract
- At the anterior perforated substance, tract divides into medial and lateral stria
- Lateral stria axons go to primary olfactory cortex – piriform region
- Medial stria carry axons across anterior commissure to opposite olfactory bulb
Clinicals:
- Anosmia – loss of sense of smell (cribriform plate fracture/ meningitis etc.)
- Olfactory hallucinations – detect smells which are not present (tumor/ Parkinson’s disease)
(II) Optic nerve: Special Somatic Afferent
- NB: covered by oligodendrocytes (not schwaan cells) and meninges
- Receptor: Rods and cones
- 1st order: Bipolar cells
- 2nd order: Ganglion cells
- Many ganglion cells inside tendinous ring pass through optic canal
- Optic nerves meet at optic chiasma at pituitary gland
- Which forms optic tract
- Goes to lateral geniculate body of thalamus
- 3rd order neuron from optic radiation to primary visual cortex
Regions where optic tract is projected:
- Lateral geniculate body
- Superior colliculus
- Pretectal nucleus
- Suprachiasmatic nucleus
Visual fields:

(III) Oculomotor nerve: General Sympathetic Efferent (eye movement) and General Viceral Efferent (parasympathetic – constriction of pupil)
(A) GSE
- From oculomotor nucleus
- Through red nucleus
- Through substantia nigra
- Exits through interpeduncular fossa
- Pierces dura mater
- Through lateral wall of cavernous sinus
- Through superior orbital fissure
- And divides into:
- Superior branch – levator palpebrae superioris and superior rectus muscles
- Inferior branch – medial rectus, inferior rectus, inferior oblique muscles
(B) GVE
- From Edinger-Westphal nucleus
- Travel in inferior branch
- To ciliary ganglion (synapse)
- Post ganglionic, short ciliary nerves pierce sclera
- Innervates:
- Spincter pupillae – smooth muscles of iris, constrict pupil
- Ciliary muscle – tighten/relax lens
Clinicals: Oculomotor nerve lesions due to:
- Increased intracranial pressure
- Aneurysm of posterior cerebral artery
- Cavernous sinus infection or trauma
Results in:
- External strabismus – eyeball down and lateral
- Ptosis – drooping upper eyelid
- Dilated pupil
(IV) Trochlear nerve: GSE (Superior oblique muscle)
- From trochlear nucleus, emerging from posterior midbrain
- Winds around brainstem
- Pierce dura of tentorium cerebelli
- Through lateral wall of cavernous sinus
- Through superior orbital fissure
- Enter orbit of eye
- Innervates superior oblique muscle
Clinicals: Trochlear paralysis – caused by vascular lesions, cavernous thrombosis, hypertension, diabetes mellitus etc.
Results in:
- Verticle diplopia – double vision
- External strabismus
(V) Trigeminal nerve: GSA and SVE
Nuclei:
- Mesenocephalic nucleus – sensory (proprioception)
- Main sensory – sensory (touch)
- Spinal nucleus – sensory (pain and temperature)
- Motor nucleus of trigeminal – motor (muscles of mastication)


Course:
- Emerges from lateral aspect of pons
- Forms trigeminal ganglion and splits into 3 branches:
V1 – Opthalmic – GSA
- Pierces dura mater
- Passes through lateral wall of cavernous sinus and superior orbital fissure
- Branches:
- Lacrimal
- Frontal (supratrochlear and supraorbital through supraorbital foramen)
- Nasociliary (short ciliary, long ciliary, infratrochlear, anterior and posterior ethmoidal)
V2 – Maxillary – GSA
- Through lateral wall of cavernous sinus and foramen rotundum
- Enters pterygopalatine fossa
- Exits via inferior orbital fissure
- Through inferior orbital groove and canal
- Exits through infra orbital foramen
- Branches:
- Meningeal
- Infraorbital (inferior palpebral, nasal and superior labial)
- Zygomatic
- Anterior, middle and posterior superior alveolar
- Pterygopalatine nerves
V3 – Mandibular – GSA, SVE
- Joins motor nerve
- Through foramen ovale
- In infratemporal fossa
Innervation:

Clinicals:
- Paralysis of muscles of mastication – due to trauma, tumor, aneurysm, meningitis, polio, multiple sclerosis, vascular lesions. Jaw deviates to side of lesion.
- Loss of sensation of soft touch, thermal and pain in face
- Loss of cornea and sneezing reflex
- Herpes zoster
(VI) Abducens nerve – GSE (lateral rectus muscle)
- Abducens nuclei
- Emerges from the ponto medullary junction
- Through cavernous sinus (medially)
- Through superior orbital fissure and common tendinous ring
- To orbit of eye
- Innervates lateral rectus – abducts eye
Clinicals: Abducens nerve lesion due to basilar or internal carotid artery aneurysms, cavernous thrombosis
Results in:
- Internal strabismus – eye down and towards nose
- Diplopia
(VII) Facial nerve: GVA, GVE, GSA, SVA, SVE
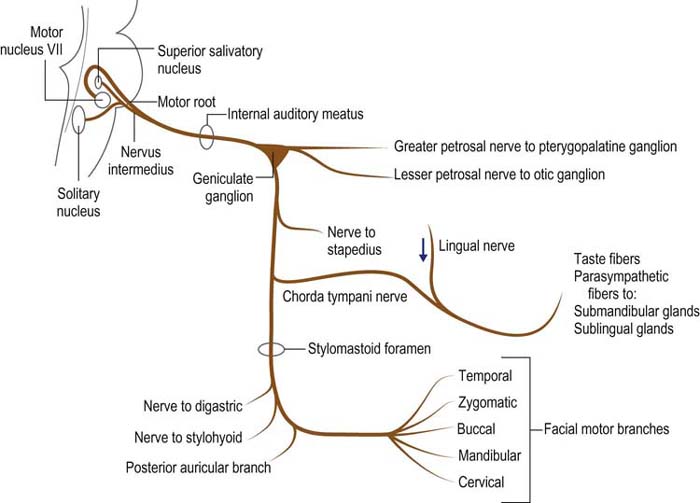
- Facial nerve is made of a motor root and intermediate nerve
- Both exit through cerebellopontine angle and internal auditory meatus
- Intermediate nerve synapses in geniculate ganglion (motor root does not)
- Both go through facial canal
- After exiting facial canal, intermediate nerve splits into:
- Greater petrosal nerve
- Chorda tympani (exits via pterygotympanic fissure)
- Motor nerve gives nerve to stapedius
- Then exits through mastoid foramen
- Gives off 3 other nerves: Posterior auricular, nerve to posterior belly diagastric and stylohyoid
- Pierces body of parotid gland and gives off the facial motor branches
Clinicals:
- Paralysis of facial nerve – ipsilateral paralysis of facial muscles
- Bells palsy

- Loss of taste – Chorda tympani, anterior 2/3 tongue
- Ipsilateral hyperacusis
- Decrease in gland production – lacrimal, sublingual, submandibular. Leads to dry eyes and dry mouth
(VIII) Vestibulocochlear nerve: SSA
- From vestibulocochlear nuclei
- Emerges from cerebellopontine angle
- Through internal acoustic meatus
- Divides into:
- Vestibular division ⇒ vestibular ganglion ⇒ hair cells etc.
- Cochlear division ⇒ spiral ganglion ⇒ spiral organ
NB: Vestibulo ocular reflex – allow images on retina to stabilize when head turns by moving eyes in opposite direction

Clinicals:
- Vestibular neuritis – inflammed vestibular nerve division. Results in vertigo, nausea, posture imbalance
- Labyrinthitis – inflammed membranous labyrinth, results in hearing loss, tinnitus (false ringing sound)
(IX) Glossopharyngeal nerve: GVA, GVE, GSA, SVA, SVE
Nuclei:

Course:
- Emerges from lateral medulla
- Leaves via jugular foramen
- Outside foramen are superior and inferior ganglia (contain cell bodies of sensory fibers)
- Branches:
- Nerve to stylopharyngeus
- Carotid sinus
- Pharyngeal branch – oropharynx mucosa
- Tonsilar branch – palatine tonsils
- Lingual branch – general and taste sensation in posterior 1/3 tongue
- Tympanic nerve ⇒ Becomes lesser petrosal nerve ⇒ Through foramen ovale ⇒ Synapse at otic ganglion which supplies to parotid gland (salivary secretion and vasodilation)
Clinicals:
- Loss of gag reflex
- Loss of taste in ipsilateral posterior 1/3 tongue
- Reduced parotid secretion – ipsilateral
- Ipsilateral weakess in swallowing
- Glossopharyngeal neuralgia – pain when swallowing or talking
(X) Vagus nerve: GVA, GVE, GSA, SVA, SVE
NB: Longest CN
Nuclei:

Course:
- Emerges from medulla of brainstem
- Gives out auricular branch (innervates external ear and external auditory canal)
- Goes through jugular foramen
- Through carotid sheath with internal jugular vein and common carotid artery
- Posterior to sternoclavicular joint, enter thorax
Branches in neck:
- Pharyngeal branches – motor to pharynx and soft palate muscle (except tensor palatine)
- Internal laryngeal nerve – Sensory to superior pharynx
- External laryngeal nerve – cricothyroid muscle
- Right recurrent laryngeal nerve – intrinsic larynx muscles
In thorax:
- Right vagus nerve forms posterior vagal trunk
- Left forms anterior vagal trunk
- Branches:
- Left recurrent laryngeal nerve – intrinsic larynx muscles
- Cardiac branches
- Contribute to oesophageal plexus
In abdomen:
- Vagal trunks enter abdomen via oesophageal hiatus in diaphragm
- In abdomen terminate by dividing into branches that supply: esophagus, stomach, small and large bowel, anterior and posterior gastric, celiac ganglion, superior mesenteric ganglion, splenic and gastric branches, pancreatic and pyloric branches, and to small and large intestines
NB: Palatoglossus innervated by vagus nerve
Clinicals:
Injury by aneurysm, cerebellopontine angle lesions, hydrocephalus, tumors, vascular lesions of brainstem
Results in:
- Dysphonia – difficulty in speaking
- Dysphagia – difficulty in swallowing
- Loss of gag reflex
- Deviation of uvula
- Hyperacidity
- Gastric ulcers
(XI) Spinal accessory nerve: SVE (sternocleidomastoid and trapezius muscle)
- Nerve from spinal accessory nucleus
- Goes through foramen magnum
- Joins with nerve from nucleus ambiguus
- Together exit jugular foramen
- Splits to innervate trapezius and sternocleidomastoid muscles
Clinicals:
- Drooping shoulders
- Assymetrical neck line
- Can’t rotate head down and away
(XII) Hypoglossal nerve: GSE (tongue muscles except palatoglossus)
- From hypoglossal nucleus
- Emerges from medulla oblongata between olive and pyramid
- Exits via hypoglossal canal
- Passes inferior to angle of mandible
- Crosses internal and external carotid arteries
- Enters tongue
Clinicals: Deviated tongue – ipsilateral
Spinal cord
Parts:

Extents: Foramen magnum to L1/L2 in adults, L3 in infants
Enlargements: Cervical (C4-T1), Lumbosacral (L2-S3)
Blood supply:
- 1 anterior spinal artery – anterior 2/3 of spinal cord
- 2 posterior spinal arteries – posterior 1/3 of spinal cord
- Radicular arteries – from ascending cervical, inferior thyroid, intercostal, lumbar and sacral arteries


Spinal veins:
- Drain into internal vertebral venous plexus (epidural)
- Which consists of anterior and posterior longitudinal venous channels – made of 6 longitudinal veins
- Also connect with external venous plexus
- Connect intracranial sinuses to superior vena cava

Contents of intervertebral foramen: Spinal nerve, dorsal root ganglion, radicular vessels, associated sympathetic plexus
Support: Spinal nerves, continuation of brain stem, denticulate ligaments (pia mater to dura mater)
Protection: Vertebral column bones, spinal meninges, CSF
Spinal nerves:
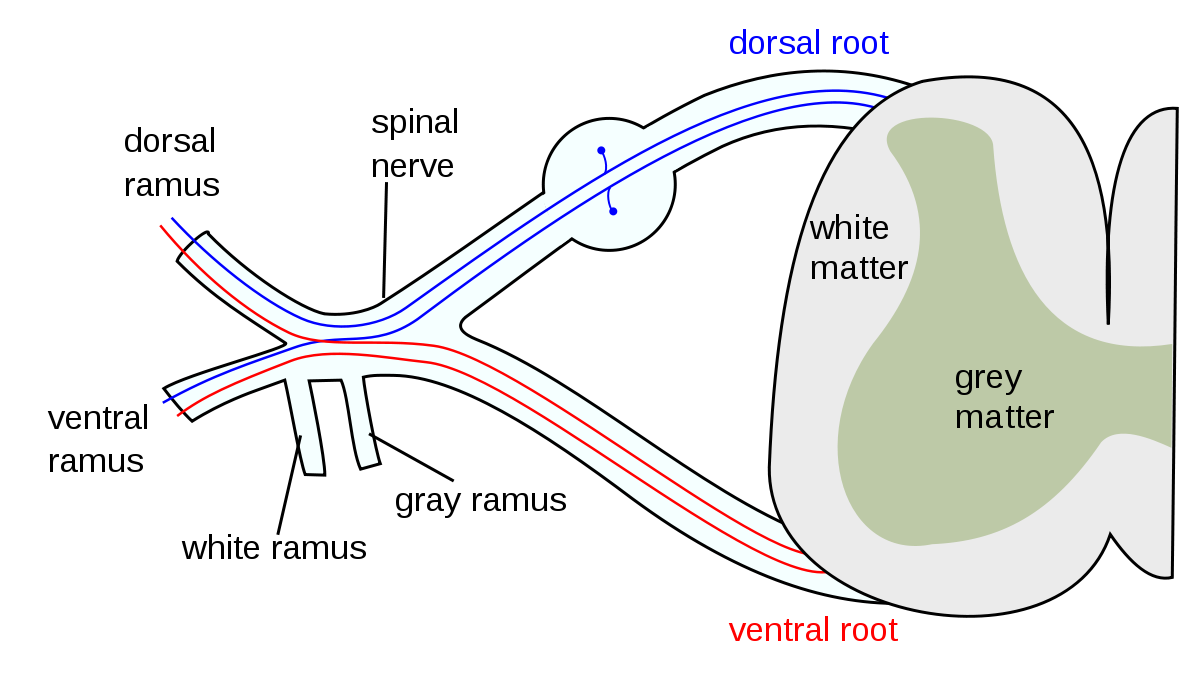
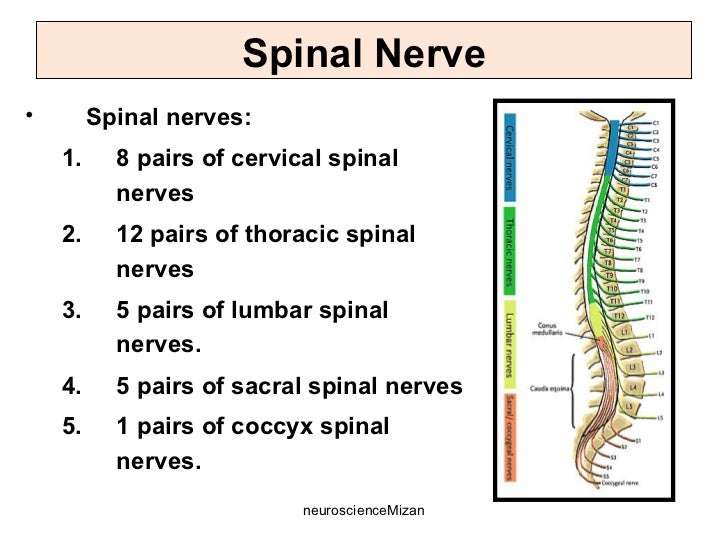
- From C1-C7, spinal nerves exit above respective vertebra
- C8 spinal nerve exits below C7 vertebra
- From T1 onwards, spinal nerves exit below their respective vertebra
- Conus medullaris – Cone shaped end of spinal cord
- Cauda equina – Nerve roots after spinal cord has ended

Dermatomes:

Spinal tracts: (Tractology in next chapter)

(I) Ascending tracts – afferent nerves
1st order – Dorsal root ganglion
- General sensation (psuedounipolar neuron) – pain, temperature, touch, pressure, vibration and proprioception
- Special sensation (bipolar neuron) – hear, vision, taste, smell, balance
2nd order:
- Synapse with 1st order in spinal cord
- Cross over
- Terminate in thalamus
3rd order:
- Synapse with 2nd order in thalamus
- Terminate in cortex
(II) Descending tracts – efferent nerves
- Upper motor – From brain to anterior horn of brainstem/spinal cord
- Lower motor – From anterior horn of brainstem/spinal cord to effectors
Spinal segments:
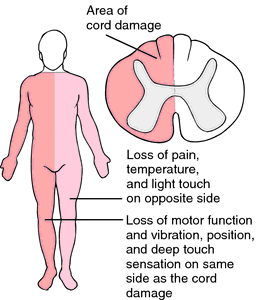
Clinicals:
- Central cord syndrome:

2. Anterior cord syndrome:

3. Posterior cord syndrome:

4. Brown sequard syndrome:
5. Chicken pox – virus can travel through sensory axons of single dermatome and erupt onto skin in a single dermatome – known as Herpes zoster/Shingles (reactivation of latet chicken pox)
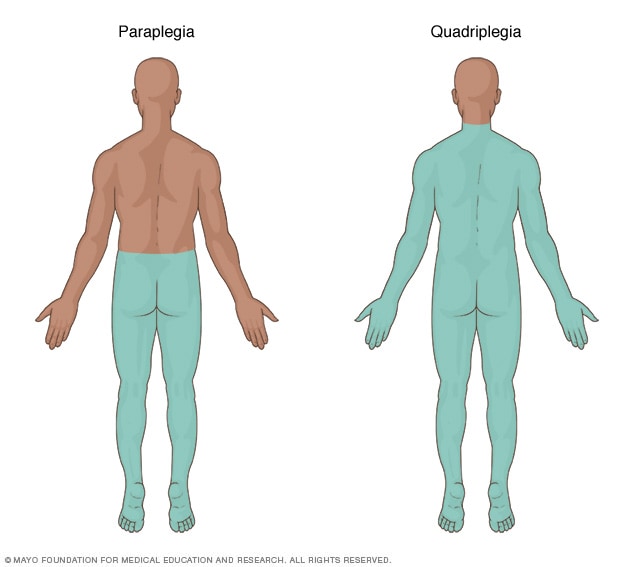
6. Quadriplegia – damage below C3; paralysis of whole trunk, arms and legs
7. Paraplegia – damage to middle spinal cord T1-L4; paralysis to legs and part of trunk
8. Lumbar cistern:
- Subarachnoid space at L3-L4 after spinal cord terminates
- Site for lumbar puncture – Patient curls so spinous process spaced. Drain CSF to diagnose meningitis.
- Pierces skin ⇒ subcutaneous tissue ⇒ thoracolumbar fascia ⇒ supraspinous ligament ⇒ interspinous ligament ⇒ epidural space ⇒ dura mater ⇒ subdural space ⇒ arachnoid mater

Cerebrum
Deep median longitudinal fissure – separates the 2 hemispheres
The main sulci – Central and lateral, divide cerebrum into frontal, parietal, temporal and occipital lobes
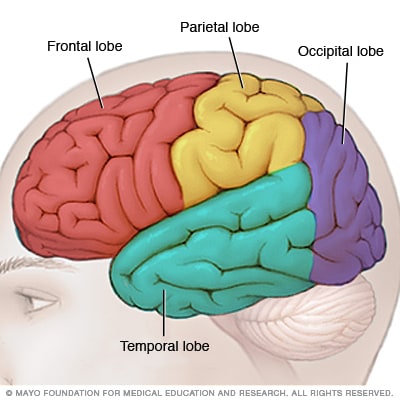
1. Frontal lobe
From central sulcus to frontal pole, from longitudinal median fissure to lateral sulcus
4 principle gyri:
- Precentral gyrus
- Superior frontal gyrus
- Middle frontal gyrus
- Inferior frontal gyrus
The lateral sulcus divides inferior frontal gyrus into:
- Pars orbitale
- Pars triangularis
- Pars opercularis
Olfactory tract divides into:
- Lateral olfactory stria
- Medial olfactory stria
2. Parietal lobe
Is divided into:
- Superior parietal lobule – somatosensory association
- Inferior parietal lobule – consists of supramarginal gyrus and angular gyrus
NB: Lower part of supramarginal gyrus forms Wernicke’s area (sensory speech)
3. Temporal lobe
On the outer bank of lateral sulcus is transverse gyri of Heschl (primary auditory area)
4. Occipital lobe
Contains primary and secondary visual cortex on either side of calcarine sulcus


Functional areas of brain:
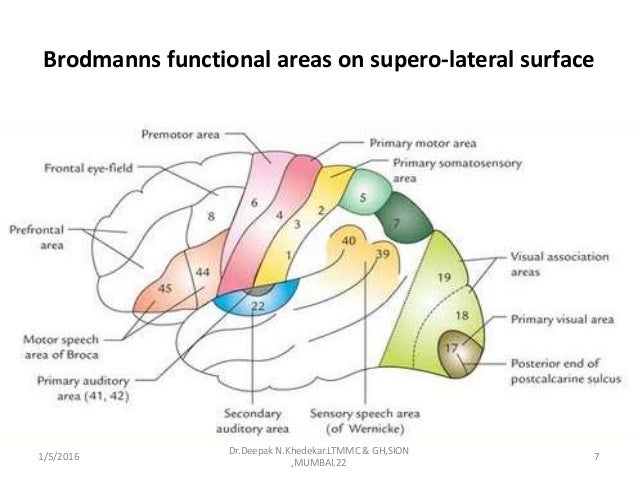
- Primary motor area – Precentral gyrus (somatic motor activity)
- Premotor area – Plans motor activity
- Prefrontal area – High CNS function (intelligence, memory, reasoning)
- Broca’s area – Motor speech (pars opercularis + pars triangularis) – if you are right handed, it is found on the left hemisphere and vice versa
- Primary sensory area – Post central gyrus (awareness of sensation)
- Wernicke’s area – Sensory or understanding speech (supramarginal gyrus)
- Primary auditory area – Transverse gyri of Heschl in superior temporal gyrus (awareness of sound)
- Secondary auditory area – Superior temporal gyrus
- Primary visual area – Both banks of calcarine sulcus
- Secondary visual area
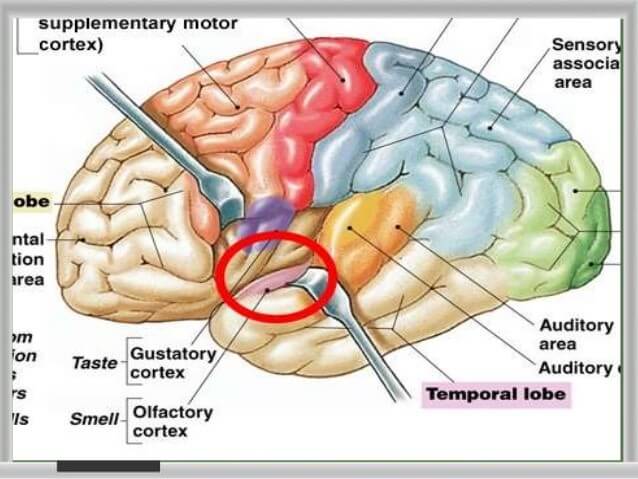
- Olfactory area – uncus (for smell)
- Gustatory area – Taste (shown in diagram)
- Horizontal eye movement – Middle frontal gyrus, middle part
Circle of Willis:
- Internal carotid artery
- Vertebral artery

Cerebrum blood supply:
(I) Anterior cerebral artery:

- Runs in callosal sulcus
- Supplies medial surface of cerebrum
Clinicals:
- Contralateral hemiplegia – Paracentral lobule: Motor and sensory loss of lower limbs
- Apraxia – Corpus callosum: Difficulty in doing tasks or learned movements
- Agnosia – Loss of sensation
- Hemihyperacusis – Increase sensitivity to sound
(II) Middle cerebral artery:
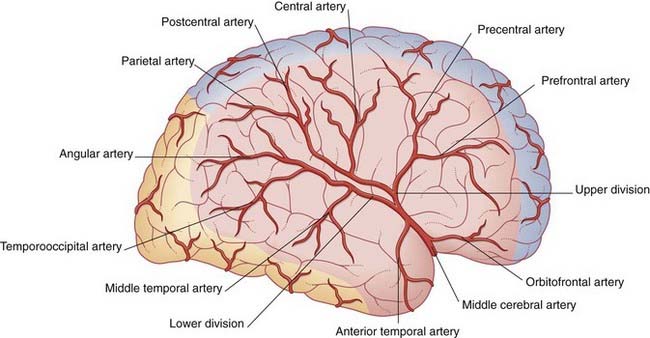
- Runs in lateral sulcus
- Supplies lateral surface of cerebrum
Clinicals:
- Contralateral loss of discriminating touch
- Contralateral hemiplegia – Motor and sensory loss of upper extremity and face
- Global aphasia – Broca’s area, Motor speech lost
- Partial deafness – Superior temporal gyrus
(III) Posterior cerebral artery:
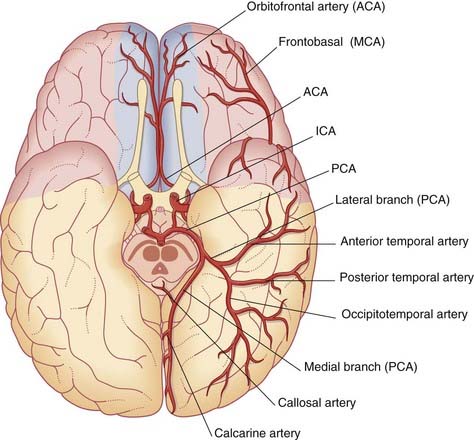
- Supplies occipital lobe, midbrain, brainstem, choroid plexus and visual cortex
Clinicals:
- Blindness
- Tunneling of vision
- Superior alternating hemiplegia/ Weber’s syndrome
Cerebral veins:
(I) Superficial cerebral veins: Run in subarachnoid space

- Superior cerebral veins – drain into superior sagittal sinus
- Superficial middle cerebral vein (runs in lateral sulcus) – drains into cavernous sinus
Also divides into:
- Superior anastomotic vein – drains into superior sagittal sinus
- Inferior anastomotic vein – drains into transverse sinus
3. Inferior cerebral vein – drains into cavernous and transverse sinus
(II) Deep cerebral veins
Basal veins (paired) and internal cerebral veins (paired) drain into great cerebral vein

Clinicals:
- Agnosia – can’t interpret sensation or recognize things
- Hemineglect – not aware of one side of body
- Visual agnosia – can’t interpret visual information
- Prosopagnosia – can’t recognize familiar faces or recall visual memories
- Apraxia – unable to perform tasks or learned movements
- Aphasia – can’t understand or express speech
- Alexia – can’t read
- Dyslexia – inability to read more than a few lines with understanding
Brain stem
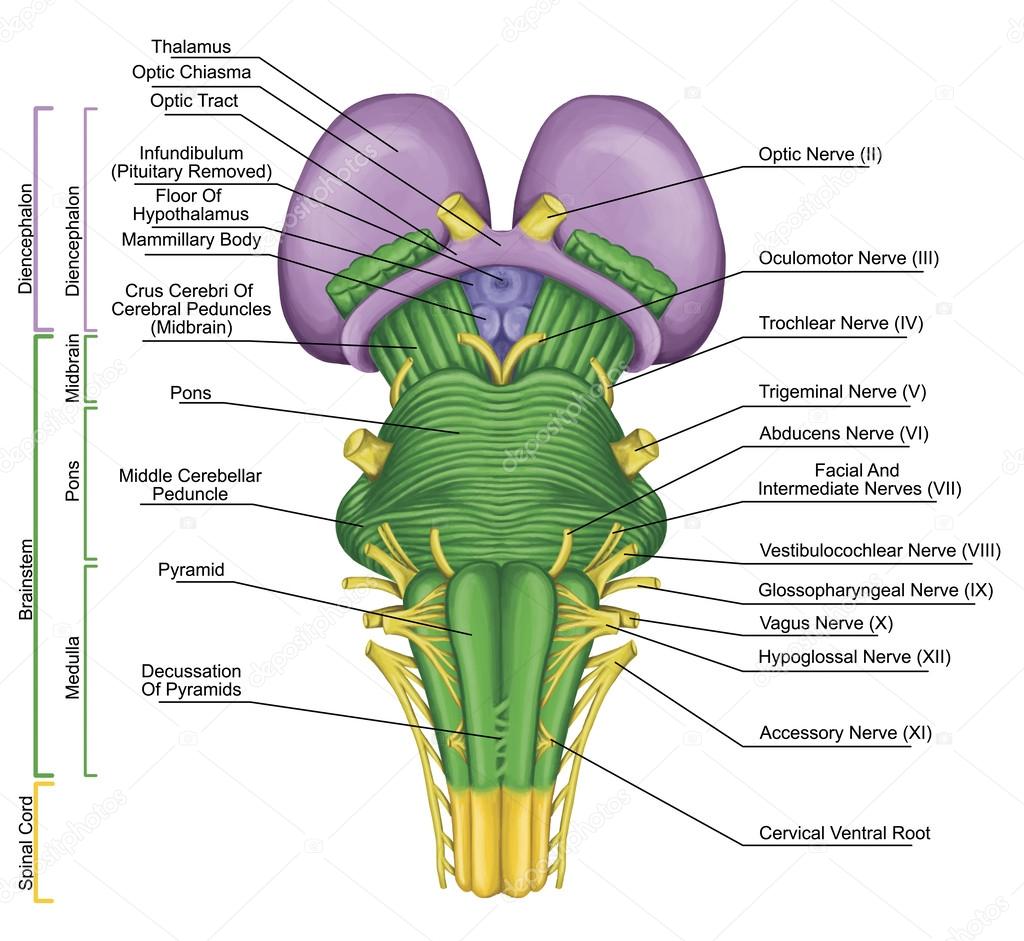
Nuclei of brain stem:

Vascular lesions of:
(I) Midbrain – Superior alternating hemiplegia/Weber’s syndrome
Occlusion of mesencephalic branch of posterior cerebral artery
- Pyramidal fibers – contralateral hemiparesis
- Occulomotor nerve – ipsilateral paralysis of occular muscles except lateral rectus and superior oblique muscles
(II) Pons – Middle alternating hemiplegia
Occlusion of pontine branches
- Corticospinal fibers – contralateral hemiparesis
- Abducens nerve – ipsilateral paralysis of lateral rectus muscle
(III) Medulla – Inferior alternating hemiplegia
A) Medial medullary syndrome
Occlusion of medullary branch of anterior spinal artery/bulbar branch of vertebral artery
- Medial lemniscus – contralateral loss of discriminating touch, vibration, position and movement sensations
- Hypoglossal nerve – ipsilateral tongue paralysis
B) Lateral medullary syndrome/ Wellenbergs syndrome
Occlusion of medullary branch of posterior inferior cerebeller artery
- Spinal lemniscus – Contralateral loss of pain and temperature
- Nucleus ambiguus – ipsilateral palate muscle paralysis in swallowing and phonation
- Trigeminal nerve – ipsilateral loss of pain and temperature on face
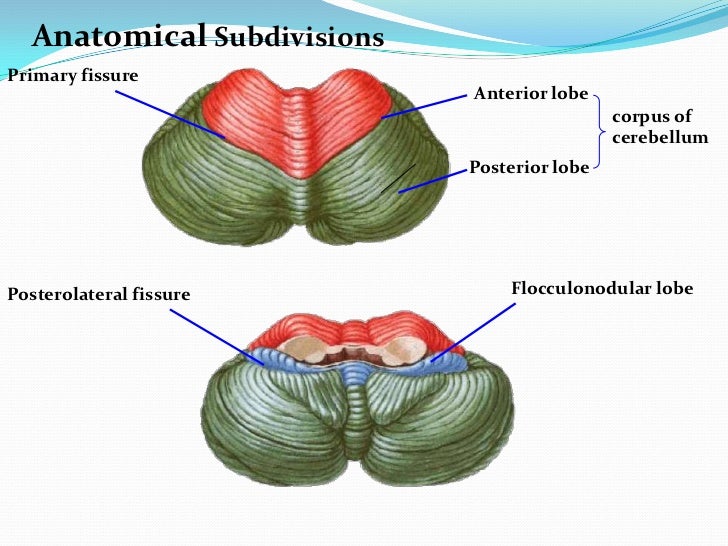
Cerebellum

Blood supply:
- Posterior inferior cerebeller artery (PICA)
- Anterior inferior cerebeller artery (AICA)
- Superior cerebeller artery (SCA)
Vein: Great cerebral vein
Nuclei:

Cerebeller peduncles:
- Superior – Midbrain
- Middle – Pons
- Inferior – Medulla
Others
1. Cerebellopontine angle:

Contents:
- Facial nerve
- Vestibulocochlear nerve
- Labyrinthine artery
Clinicals: Cerebellopontine tumor – compress nerves, cerebellum and pyramids
2. Interpeduncular fossa:

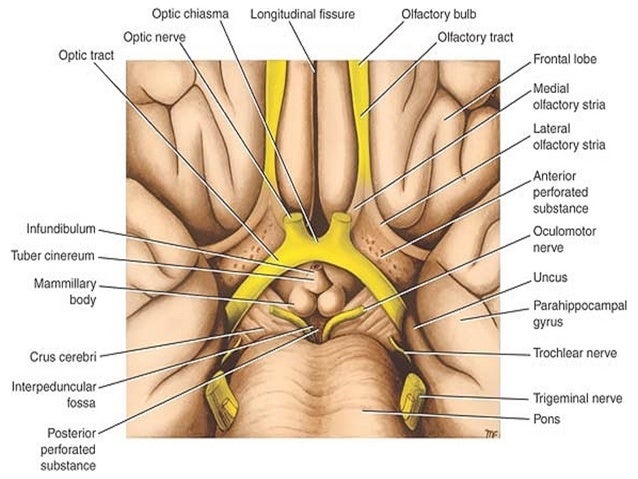
Contents:
- Mammillary bodies
- Occulomotor nerve
- Infundibulum stalk
- Tuber cinereum
- Posterior perforated substance
Clinicals: Tumors – compress nerves, hypothalamus and crus cerebri
3. Pineal body:
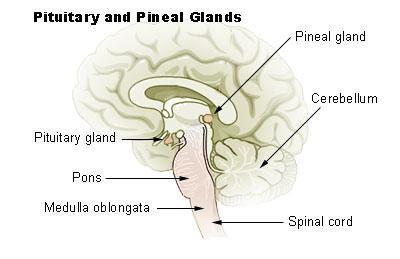
Relations:
- Laterally – Cerebral hemispheres (thalamic bodies)
- Rostrally: Wall of 3rd ventricle
- Inferiorly: Superior colliculus
Functions:
- Produce melatonin
- Regulate circadian rhythm
- Modulation of sleep patterns
- Delays puberty
- Neuroendocrine transducer
Clinicals:
- Vertical gaze palsy – can’t move eyes up, pineal gland tumor
- Pseudopuberty precocious
4. Corpus callosum

Blood supply:
- Pericallosal artery
- Subcallosal artery
- Median callosal artery
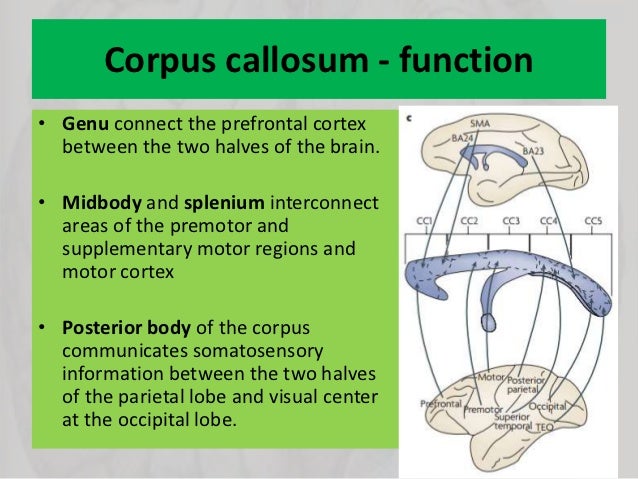
5. Commissural fibers:
Connect the 2 hemispheres of the brain:

6. Association fibers:


7. Cavernous sinus:


Relations:
- Superior – Temporal lobe
- Inferior – Sphenoid air sinus
- Medial – Pituitary gland
- Lateral – Trigeminal ganglion
- Anterior – Optic nerve
- Posterior – Petrous temporal bone
Contents: Internal carotid artery, CN 3, 4, 5-1, 5-2, 6
Clinical: Spread of infection, cavernous sinus thrombosis
NB: Drains in pterygoid plexus
8. Pituitary gland:
Location: On sella turcica
Relations:
- Superior – Optic chiasma
- Inferior – Sphenoid air sinus
- Lateral – Cavernous sinus
- Anterior – Spenoid air sinus
- Posterior – Dorsum sellae
Clinical: Pituitary tumor – endocrine dysfunction
9. Diencephalon:

(I) Thalamus:
Relations:
- Superior – Floor of lateral ventricle
- Inferior – Hypothalamus
- Medial – 3rd ventricle
- Lateral – Internal capsule
Blood supply: Posterior communicating, posterior cerebral, anterior choroidal
Nuclei:

(II) Hypothalamus:
Relations:
- Superior – Thalamus
- Inferior – Optic chiasma
- Anterior – Frontal lobe
- Posterior – Midbrain
- Lateral – Internal capsule
- Medial – 3rd ventricle
10. CSF and ventricular system:

Production and flow of CSF:
- Choroid plexus in lateral ventricle produces CSF
- Flows in 3rd ventricle via intraventricular foramina
- To 4th ventricle via cerebral aqueduct
- Flows into subarachnoid space over brain and spinal cord vis paired lateral foramina of Lushka and median foramen of Magendi
- Resorption into venous sinus by arachnoid granulations in superior sagittal sinus
- Flows by pulsation of spinal arteries
Functions of CSF:
- Cushion brain
- Support brain weight
- Provide nutrients, remove waste
- Integration of endocrine functions
11. Basal ganglia: Deep nuclei of cerebrum which regulate motor activity
- Caudate nucleus
- Putamen
- Globus pallidus – Medial and Lateral
- Subthalamic nucleus
- Substantia nigra
- Striatum: Caudate nucleus and putamen
- Lentiform nucleus: Putamen and globus pallidus
12. Horizontal cross section of cerebrum:


13. Papez circuit of emotions:

These are summarized notes from various sources, mainly TeachMeAnatomy and Wikipedia

1 thought on “Neuroanatomy and Cranial Nerves”
Comments are closed.