Midgut
Origin: Endodermal

- Cranial limb – forms jejunum and ileum
- Caudal limb – forms ascending colon and 2/3 of transverse colon
- Cecal swelling – forms cecum, appendix and part of ascending colon
- Intestinal loop elongates rapidly and leaves the small abdominal cavity and enters umbilical cord – physiological umbilical hernia (6th to 10th week)
- The elongating loop rotates 270 degrees anticlockwise around axis of superior mesenteric artery (seen in the diagram)
- Therefore upper part of small intestine lies behind colon
- 10th week, abdominal cavity enlarges and :
- Jejunum reenters to left side
- Ileum reenters to right side
- Cecal swelling reenters below liver
- Cecal swelling elongates downwards to right iliac fossa – forms right colic flexure and ascending colon
- Vitellointestinal duct obliterated
Congenital anomalies:
- Remnant of vitelline duct:
- Meckel’s diverticulum – proximal part near ileum remains patent
- Vitelline fistula – whole vitelline duct remains open
- Vitelline cyst – Middle part remains open

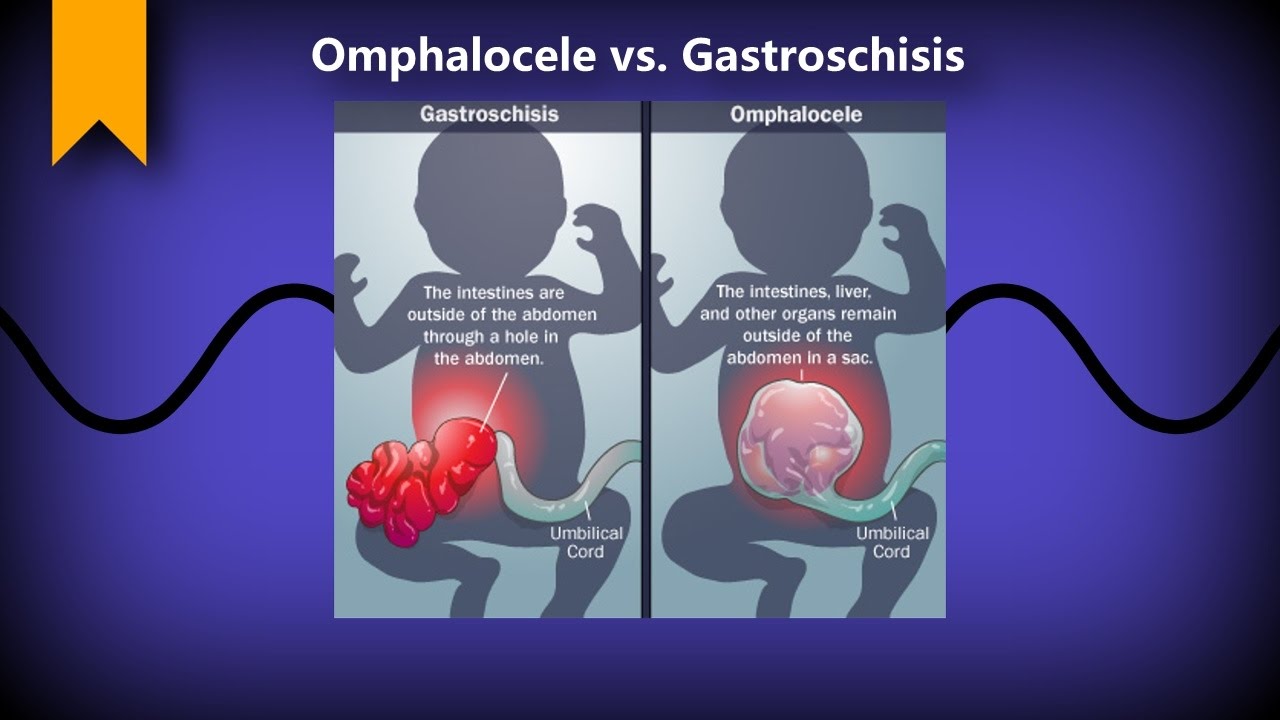
2. Omphalocele/ Congenital umbilical hernia – Failure of reduction of physiological hernia due to defect in abdominal wall muscles development
3. Gastroschisis
4. Atresia/ stenosis of any part of primitive intestinal loop – bowel obstruction
5. Abdominal rotation of intestinal loop – 90 degrees only or clockwise rotation
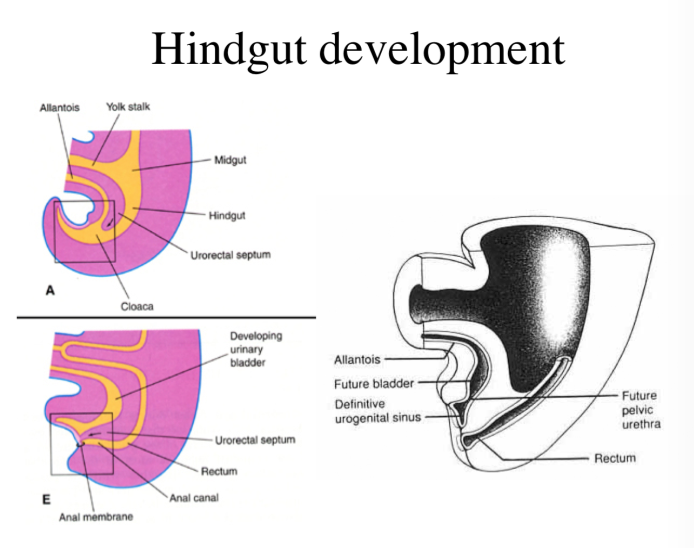
Hindgut
Origin: Endodermal
Derivatives: Left 1/3 transverse colon, descending colon, sigmoid colon, rectum, upper 1/2 anal canal (Lower 1/2 anal canal, proctodeum – ectodermal)
- Lower end of hindgut dilates to form cloaca
- And then continues as allantois to umbilicus
- Below cloaca is cloacal membrane
- Which is bilaminar: outer ectoderm, inner endoderm
- Between hindgut and allantois is a urorectal septum, which grows caudally and divides the cloaca and cloacal membrane into:
- Primitive urogenital sinus (ventrally) – Urogenital membrane
- Rectoanal canal (dorsally) – anal membrane
- Opposite rectoanal canal, ectodermal depression called proctodeum forms
- Anal membrane ruptures:
- Proctodeum – lower 1/2 anal canal
- Rectoanal canal – rectum and upper 1/2 anal canal
Congenital anomalies:
- Imperforate anus – anal membrane fails to rupture
- Atresia of rectum – Proctodeum fails to develop
- Stenosis of rectum – incomplete canalization
- Recto – vaginal fistula, recto – urinary fistula, recto – urethral fistula – incomplete division of cloaca
- Anal atresia, anal stenosis
- Ectopic anus
