Bones and how to side them
Vertebra:
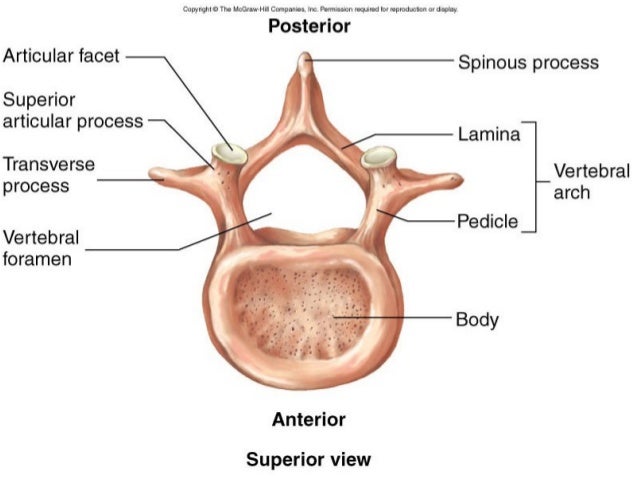
Types of vertebra:

Atlas (C1) – no body, no spinous process, dens foramen, transverse foramen, anterior and posterior arch and tubercle
Axis (C2) – dens, bifid spine, transverse foramen
Cervical vertebra – bifid spine (C7 is long and not bifid), transverse foramen and horizontal articular facets
Thoracic vertebra – vertical articular facets, heart shaped body, spine long and downwards
Lumbar vertebra – sagittal articular facets, kidney shaped body

Vertebral ligaments:
- Anterior longitudinal – prevent hyper extension
- Posterior longitudinal – prevent hyper flexion
- Ligamentum flavum – prevent abrupt flexion (between laminas)
- Interspinous
- Supraspinous
- Intertransverse ligament

- Static stability of vertebral column – ligaments
- Dynamic – back muscles ie. iliocostalis, longissimus, spinalis (from lateral to medial)
NB: Vertebral column divided into 3 vertical parallel columns:

Anterior column:
- Anterior longitudinal ligament
- Anterior 2/3 of vertebral body
- Anterior 2/3 of intervertebral disc (annulus fibrosus)
Middle column:
- Posterior 1/3 of vertebral body
- Posterior 1/3 on intervertebral disc
- Posterior longitudinal ligament
Posterior column:
- Ligament flavum
- Pedicles
- Facet joints and articular processes
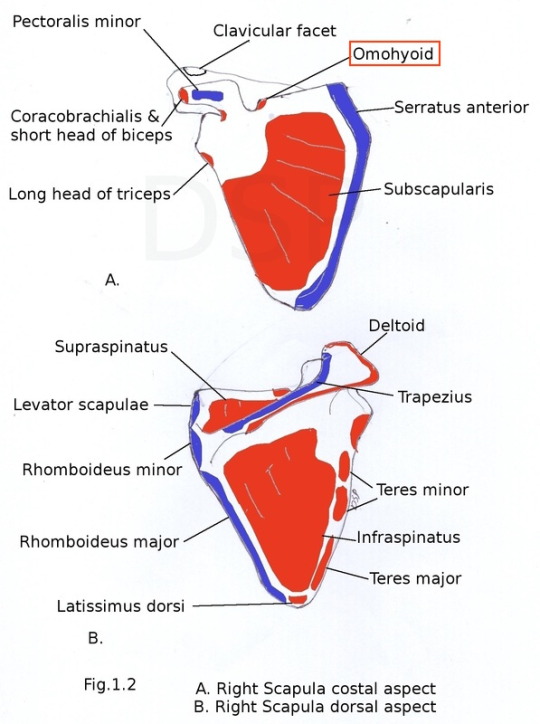
Scapula:

Clavicle:
- Acromial/lateral end is flat
- Sternal/medial end is thick and round
- Superior surface is smooth, inferior surface is rough
- Medial curve protrudes outward

Unique features of clavicle:
- Ossifies during week 5 (fetal) and completed at 25 years, others ossify at week 8 and complete at 18-21 years
- Runs a sigmoid, horizontal course
- No marrow cavity, core occupied by spongy bone
- Medial 2/3 ossify endochondrally, lateral 1/3 intramembranously
Functions of clavicle:
- Hold upper limb away from trunk and increase range of movement such as abduction
- Transmit weight from upper limbs to axial skeleton
- Provide attachment for muscles
Clinicals:
- Fracture between medial 2/3 and lateral 1/3
- Lateral fragment pulled medial and forward by pectoralis major
- Injury to brachial plexus and axillary vessels
- Injury to subclavian artery
Sternum:

Sternal angle – angle formed by the junction of manubrium and body of sternum.
Importance: landmark to indicate level at which the 2nd rib joint with the sternum
Humerus:
- Medial epicondyle more outwards than lateral
- Lateral side – capitulum and deltoid tuberosity

Radius:
- Anterior surface smooth and concave at lower end
- Laterally – convex, lateral styloid process
- Medially – ulnar notch and medial tuberosity
- Lower end is large

Ulna:
- Medial styloid process
- Convex medially

Bones of hand:

From thumb to little finger:
- Trapezius, trapezoid, capitate, hamate
- Scaphoid, lunate, triquetral, pisiform
Muscle attachment on bones





Clinicals:
- Dropped shoulder – trapezius paralyzed
- Winged shoulder – serratus anterior paralyzed
Arteries

NB: Same for deep veins of the arm, all deep veins are venae commitantes with the arteries.
(I) Axillary artery – chest, axilla, breast and shoulder joint
- Continuation of subclavian artery from lateral border of first rib
- Divided into 3 parts by passing posterior to pectoralis minor:
- 1st part – Superior thoracic
- 2nd part – Thoracoacromial and lateral thoracic
- 3rd part – Anterior circumflex humeral, posterior circumflex humeral, subscapular
- Continues as brachial artery from inferior border of teres major
(II) Brachial artery – all arm muscles and elbow joint
- Descends on ventral surface
- Medial to humerus
- Median nerve crosses over it from lateral to medial
- At apex of cubital fossa, divides into radial and ulnar arteries
- Other branches: profunda brachii (which gives middle and radial collateral), superior and inferior ulnar collateral and humeral nutrient artery
(III) Ulnar artery – anterior forearm muscles
- Descends obliquely on ulnar side and runs along ulnar border to wrist
- Deep to pronator teres
- Deep to superficial and intermediate muscles
- Lateral to ulnar nerve
- Superficial to flexor retinaculum
- Through Hook of Hamate and Guyon’s canal
- Divides into superficial and deep palmar arch
- Branches: anterior and posterior ulnar recurrent, common interosseous
(IV) Radial artery – posterior forearm muscles
- Descends obliquely on radial side and runs along radial border
- Anterior to pronator teres
- Winds around head of radius to go posterior
- Medial to radial nerve
- Through anatomical snuff box
- Divides into superficial and deep palmar arch
Veins
Superficial veins of arm:

NB: Cephalic V. used for:
- Drawing of blood
- Intravenous injection
- Venous cutdown
Nerves
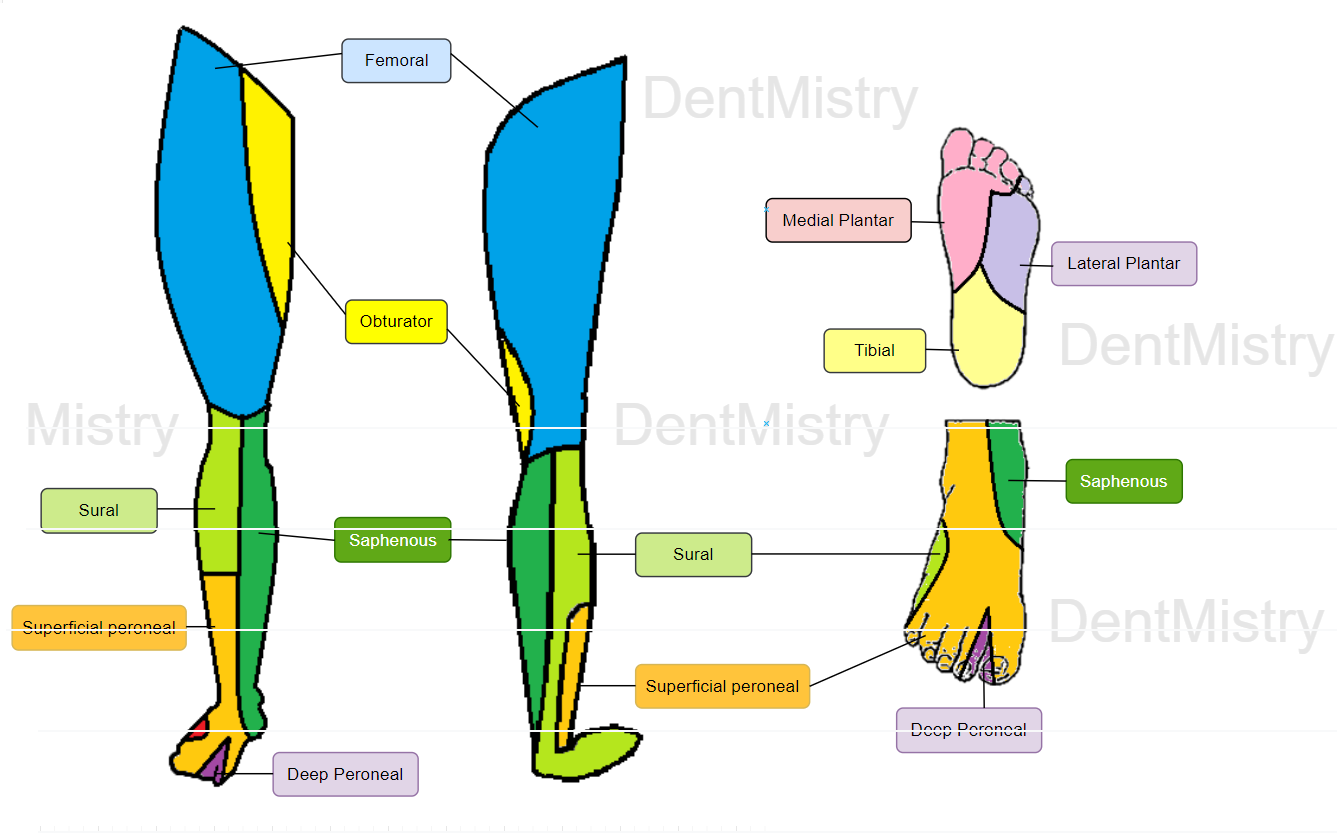
Cutaneous innervation of upper limbs:


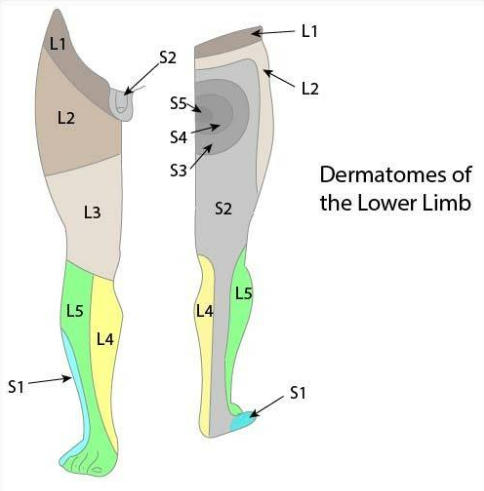
Dermatomes of upper limbs:


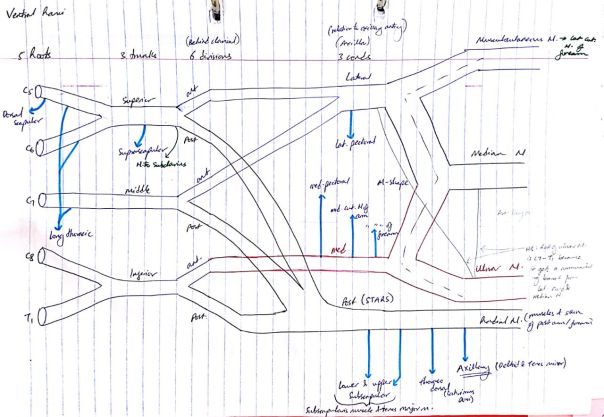
(I) Musculocutaneous nerve – anterior arm muscles, lateral forearm skin
- Roots – C5, C6, and C7
- At inferior border of pectoralis minor
- Pierce coracobrachialis muscle
- Runs between brachialis and biceps brachii
- Becomes lateral cutaneous nerve of forearm
- Runs in cubital fossa with cephalic vein
(II) Median nerve – anterior forearm muscles except flexor carpi ulnaris, elbow and wrist joint
- Roots – C5-T1
- The 2 cords join in axilla to form median nerve
- Crosses over brachial artery from lateral to medial
- Through cubital fossa
- Between 2 heads of pronator teres
- Through carpal tunnel
- Divides into recurrent and palmer digital nerves
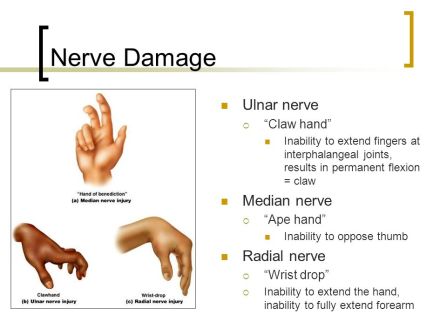
Clinical: Carpal tunnel syndrome, hand of Benediction/ monkey hand
Entrapments: Carpal tunnel, cubital fossa, pronator teres heads
(III) Ulnar nerve – elbow joint, flexor carpi ulnaris and flexor digitorum profundus muscles
- Roots – C8-T1
- Runs in medial arm
- Passes posterior to medial epicondyle at elbow
- Between 2 heads of flexor carpi ulnaris
- Travels on the ulna side
- Superficial to flexor retinaculum
- Through hook of Hamate and Guyon’s canal
- Divides into superficial and deep branches
Clinical: Ulnar claw, fracture at medial epicondyl
Entrapments: Cubital tunnel, Guyon’s canal, flexor carpi ulnaris 2 heads
(IV) Radial nerve – Posterior arm and forearm muscles and skin
- Roots – C5-T1
- Posterior to axillary artery in axilla
- Posterior to brachial artery
- Between long and medial head triceps
- Exists via lower triangular space with profunda artery
- Runs in radial groove of humerus
- Pierce lateral intermuscular septum
- Anterior to lateral epicondyle of humerus
- Through cubital fossa
- Winds around neck of radius
- Penetrates supinator
- Descends between superficial and deep muscles of the posterior forearm
- Lateral to radial artery in anatomical snuff box
Clinicals:
- Injury in axilla/ humerus fracture – elbow, wrist and finger drop
- Injury in radial groove – wrist and finger drop
- Injury in radial head fracture – finger drop
- All have loss of sensation
Entrapments: Axilla, lower triangular space, radial groove, cubital fossa, anatomical snuff box
NB:
- Brachialis muscle supplied by both radial and musculocutaneous nerves
- Flexor digitorum profundus supplied by both ulnar and median nerves
(V) Axillary nerve – Glenohumeral joint, teres minor and deltoid muscle, skin of superolateral arm
- Roots – C5-C6
- Exists axilla via quadrangular space (with posterior circumflex humeral)
- Posterior division supplies teres minor
- Anterior division winds around neck of humerus – supplies anterior part of deltoid
Clinicals:
- Fracture of surgical neck
- Entrapment in quadrangular space
- Glenohumeral joint dislocation
- All this leads to paralysis of deltoid and teres minor and loss of skin sensation
Entrapments: Shoulder dislocations, axilla, quadrangular space
Joints
(I) Glenohumeral/shoulder joint
Classification: Ball and socket synovial
Articular surfaces: Head of humerus and glenoid fossa
Stability factors:
- Static: Coracoacromial arch (prevent superior displacement), coracoacromial ligament, glenohumeral ligament
- Dynamic: Rotator cuff muscles, deltoid, trapezius
Movements: Flexion, extention, abduction, adduction, medial and lateral rotation

NB: For abduction:
- 0 – 15 degrees – supraspinatus
- 15 -90 degrees – deltoid middle part
- 90 – 120 degrees – infraspinatus, teres minor
- 120 – 180 degrees – trapezius and serratus anterior
Blood supply: Anterior and posterior circumflex humeral
Nerve supply: Axillary, suprascapular
Clinicals: Due to shallow fossa, pulled anterior and inferior, damages axillary nerve
NB: Glenohumeral joint capsule has opening for biceps tendon
(II) Elbow joint
Classification: Synovial uniaxial hinge
Articular surfaces:
- Trochlea – trochlea notch on ulna
- Capitulum – head of radius
Stability factors:
- Static: Annular ligament, radial and ulnar collateral ligaments

2. Dynamic: Triceps, biceps, brachialis and radiobrachialis
Movements: Flexion and extension
Blood supply: Elbow anastomosis (written in arteries)
Nerve supply: Musculocutaneous, radial and ulna
Clinicals: Bursitis, dislocation, golfers elbow (medial epicondylitis), tennis elbow (lateral epicondylitis)
(III) Radioulnar joint
Proximal:
Classification: Synovial pivot uniaxial
Articular surfaces: Head of radius, radial notch on ulna
Stability factors: Annular ligament
Movements: Supination and pronation
Nerve supply: Musculocutaneous, median, radial and ulna
Distal:
Classification: Synovial pivot uniaxial
Articular surfaces: Ulna head and ulnar notch on radius
Movements: Supination and pronation
Blood supply: Anterior and posterior interosseous
Nerve supply: Anterior and posterior interosseous
Clinicals: Subluxation of radial head
(IV) Wrist joint
Classification: Ellipsoid synovial
Articular surfaces: Scaphoid, lunate, articular disc and distal end of radius
Stability factors:
1. Static: Joint capsule and ligaments:
- Palmer radiocarpal
- Dorsal radiocarpal
- Ulnar collateral – styloid process to trapezoid and pisiform
- Radial collateral – styloid process to scaphoid and trapezius
2. Dynamic: Carpal tunnel contents

Movements: Flexion, extension, abduction and adduction
Blood supply: Dorsal and palmer carpal arches
Nerve supply: Median nerve
Clinicals: Anterior lunate dislocation, carpal tunnel syndrome
(V) Sternoclavicular joint
Classification: Synovial saddle
Articular surfaces: Clavicle sternal end, manubrium of sternum, 1st costal cartilage
NB: Covered in fibrocartilage, separated into 2 compartments by articular disc
Stability factors: Anterior and posterior sternoclavicular ligament, interclavicular ligament, costoclavicular ligament

Clinicals: Anterior and posterior dislocations
(VI) Acromioclavicular joint
Classification: Plane synovial
Articular surfaces: Lateral end clavicle and acromion
NB: Covered in fibrocartilage, separated into 2 compartments by articular disc
Stability factors: Acromioclavicular ligament
Movements: Anterior and posterior
Clinicals: Suspend weight from upper limb from clavicle, dislocation

Others
1. Intervertebral disc – hyalin cartilage, shock absorber, hold adjacent vertebra together, distributes weight transmission
Clinicals: prolapsed IVD, herniation of IVD

2. Primary curvature – Kyphosis – thoracic and sacral
Secondary curvature – Lordosis – Cervical and lumbar

Clinical: Scoliosis

3. Mammary glands:
Extent:
Medially Laterally
2nd rib
Sternum ———-Mid axillary line
6th rib
- Axillary tail extends into axilla laterally
- Nipple at 4th intercostal space
Relations: overlies pectoral fascia covering 4 muscles
- Pectoralis major
- Serratus anterior
- External abdominis aponeurosis
- Rectus abdominis
Separated from fascia by retromammary space with loose connective tissue. This is the basis for free mobility of the breast chest wall
Base of breast ⇒ Retromammary space ⇒ Pectoral fascia
Blood supply:
- Perforationg branches of lateral thoracic
- Perforating branches of posterior intercostal arteries
- Superior thoracic
- Thoracoacromial
Nerve supply: 4th to 6th intercostal nerves
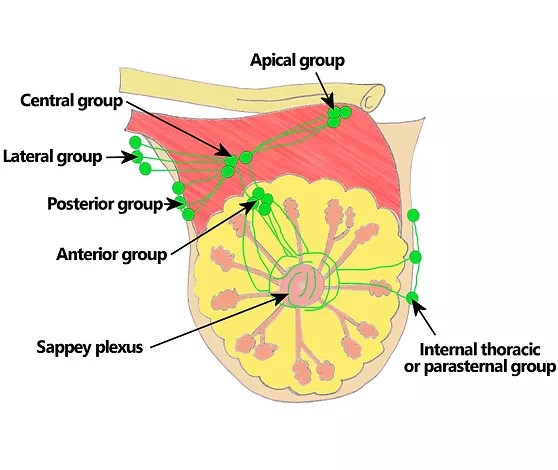
Lymphatic drainage:
- Internal mammary/ Internal thoracic
- Axillary (anterior, posterior, lateral and central)
- Supraclavicular nodes
Clinicals:
- Breast cancer – spread via lymphatics/venous channels. Due to axillary tail, axillary lymph nodes in breast cancer examined – swollen axillary nodes
- Mammography – radiography of breasts
- Masectomy – breast removal
- Mastities – infection through nipple during lactation
- Peau d’orange – ridges due to edema, inverted nipple
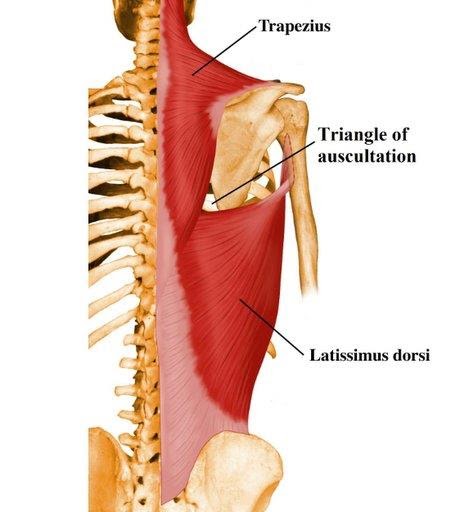
4. Triangle of auscultation – hear respiratory sounds
- Trapezius
- Scapular border
- Latissimus dorsi
5. Deltopectoral triangle:

Contents: Cephalic vein and thoracoacromial branch
6. Clavipectoral fascia – fills gap between pectoralis minor and clavicle

7. Rotator cuff:
- Supraspinatus
- Infraspinatus
- Subscapularis
- Teres minor

Clinicals:
- Rotator cuff tendinitis (inflamed tendons)
- Rotator cuff tear (supraspinatus)
8. Spaces of the arm:

- Quadrangular space – Axillary nerve and posterior humeral circumflex vessels
- Upper triangular space – Circumflex scapular vessels
- Lower triangular space – Radial nerve and profunda brachii vessels
Clinicals: Entrapment syndrome
9. Axilla:

Boundaries:
- Anterior wall: Pec minor, pec major and clavipectoral fascia
- Medial wall: Serratus anterior, intercostal muscles, 1-4 ribs
- Lateral wall: Coracobrachialis, short head biceps brachii
- Posterior wall: Subscapularis, teres major, latissimus dorsi
- Base: Skin and fascia
- Apex:
- Anterior – clavicle
- Posterior – superior border scapula
- Medial – 1st rib
Contents:
- Axillary artery and vein
- Brachial plexus cords
- Axillary lymph nodes
- Axillary tail of breasts
Clinicals: Aneurysms, lymphomas
10. Cubital fossa:
Boundaries:

Contents: Medial to lateral
- Median nerve
- Brachial artery
- Biceps brachii tendon
- Radial nerve
Mnemonic: My Bottoms Turned Red
Clinicals:
- Brachial pulse
- Venepuncture – median cubital vein
- Cubital fossa syndrome
11. Carpal tunnel:
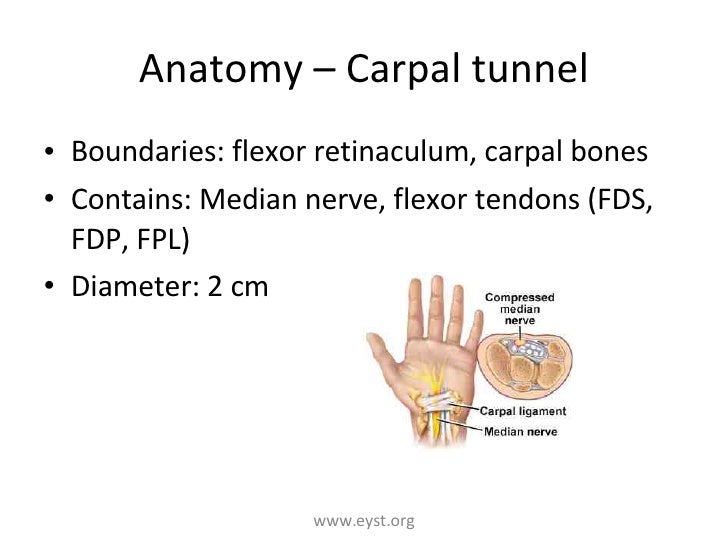
Anterior relations – Ulnar nerve and artery, palmaris longus tendon
Clinicals: Carpal tunnel syndrome – compressed median nerve, swollen tendons, thickened ligaments. Feelings of numbness and tingling
12. Anatomical snuff box:
Boundaries:
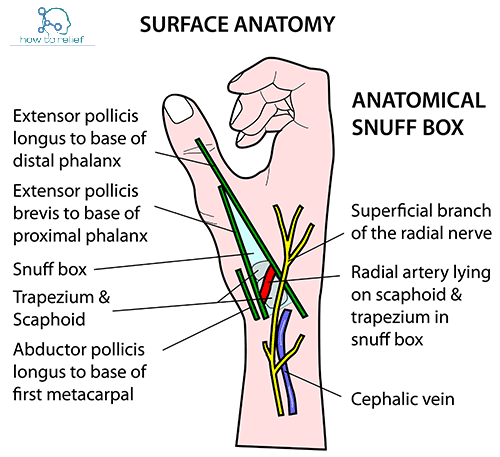
Floor – Scaphoid and trapezium
Contents:
- Radial artery
- Branch of radial nerve
- Cephalic vein
Clinical: Scaphoid fracture (arthritis, avascular, necrosis)
These are summarized notes from various sources, mainly TeachMeAnatomy and Wikipedia