Category Archives: Gross Anatomy
Female reproductive system
External genitalia/ Vulva
Blood supply: Pudendal arteries
Venous: Labial veins – drain to pudendal veins
Nerves: Urogenital plexus
- Anterior – ilioinguinal and genital branch
- Posterior – pudendal and posterior cutaneous nerves of thigh
Lymphatics: Superficial inguinal, deep inguinal (glans clitoris)
Clinicals:
- Infection of Bartholin’s glands
- STD
- Vulvar trauma – disruption of vessels
Uterus
Location: Posterosuperior to bladder , anterior to rectum
Supports:
- Pelvic diaphragm and urogenital diaphragm – main support
- Broad ligament – sides of uterus to pelvis
- Round ligament – uterine horns to labia majora via inguinal canal
- Ovarian ligament – ovaries to uterus
- Cardinal ligament – from cervix to lateral pelvic walls, contains uterine vessels
- Uterosacral ligament – cervix to sacrum
- Pubocervical ligament – cervix to pubic symphysis
Relations:
- Anterior – Uterovesical pouch, superior surface bladder
- Posterior – Rectouterine pouch, sigmoid colon
- Lateral – Broad ligament, uterine vessels
Blood supply: Uterine and ovarian arteries
Venous: Uterine venous plexus
Nerves: Pelvic splanchnic and lumbar – inferior hypogastric plexus
Lymphatics: Iliac and sacral
Clinicals:
- Hysterectomy – surgical removal of uterus
- Cervical cancer
- Endometriosis – ectopic endometrial tissue usually at ovaries and uterus ligaments
- Fibroids – benign tumors, can cause pelvic pain and infertility
- Endometrial carcinoma – often during or after menopause
Vagina
Relations:
- Anterior – Bladder fundus and urethra
- Posterior – Rectum, anal canal, rectouterine pouch
- Lateral – Ureter, uterine artery, levator ani
Blood supply: Uterine and vaginal arteries
Venous: Vaginal veins drain into vaginal venous plexus
Nerves:
- Autonomic: Uterovaginal nerve plexus (from inferior hypogastric plexus)
- Somatic: Deep perineal nerve (from pudendal nerve)
Lymphatics: Iliac and superficial inguinal lymph nodes
Clinicals:
- Vaginal infections – candidiasis and bacterial vaginosis (during pregnancy, diabetes, antibiotic treatment)
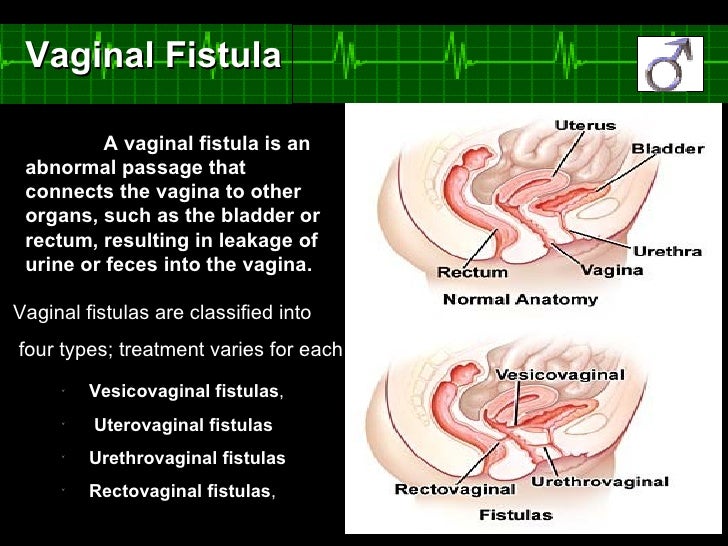
- Vaginal fistula – due to long and traumatic childbirth
Ovaries
Location: Ovarian fossa, posterior wall of broad ligament
Support:
- Mesovarium – part of broad ligament
- Suspensory ligament of ovary – contains neurovascular srtuctures
- Ovarian ligament
Blood supply: Uterine and ovarian arteries
Nerves:
- Sympathetic: Ovarian plexus
- Parasympathetic: Uterine plexus
Lymphatics: Paraaortic nodes
Clinicals:
- Ovarian cyst
- Tumors
- Polycystic ovary syndrome – elevated male hormones, irregular/no periods, body and facial hair
Fallopian tubes

Location: Upper border of broad ligament, from uterus to abdominal cavity
Blood supply: Tubal branches of uterine and ovarian arteries
Nerves:
- Sympathetic: Ovarian plexus
- Parasympathetic: Uterine plexus
Lymphatics: Iliac, sacral, aortic nodes
Clinicals:
- Ligation of uterine tubes – sterilization
- Ectopic pregnancy
- Salpingitis – inflammation due to bacterial infection
These are summarized notes from various sources, mainly TeachMeAnatomy and Wikipedia
Male reproductive system
Arteries

Scrotum
Coverings:
- Skin (dark, rugae, thin)
- Superficial fascia (no fat)
- Darto’s muscle
NB: When cold, Darto’s muscle contracts skin, scrotum wrinkles and therefore reduces surface area for heat loss
Scrotum divided internally by Darto’s fascia into left and right, externally seen as scrotal raphe
Location: Inferior and posterior to penis
Contents: Testis, epididymis, spermatic cord
Blood supply: Anterior scrotal, posterior scrotal, cremasteric
Venous: Scrotal veins drain into external pudendal veins
Nerves:
- Genitofemoral nerve – genital branch
- Ilioinguinal nerve – anterior scrotal nerve
- Pudendal nerve – posterior scrotal nerve
- Posterior femoral cutaneous – perineal branch
Lymphatics: Superficial inguinal nodes
Testis
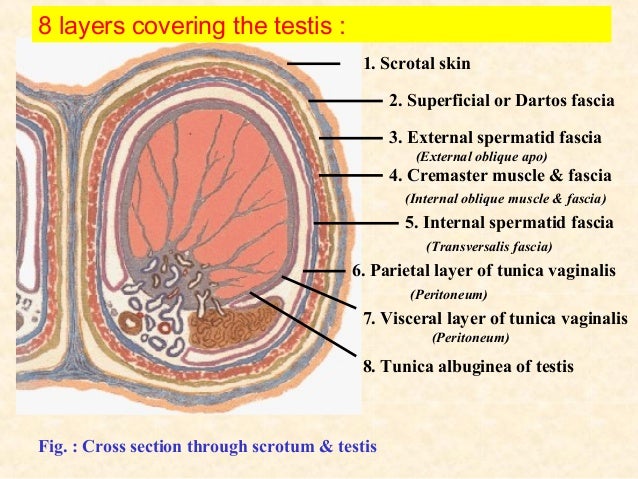
Coverings:
Blood supply: Testicular, scrotal, deferential, cremasteric
Venous: Right testicular vein drains into IVC, left drains into left renal vein
Nerves: Testicular plexus
Lymphatics: Lumbar nodes
Clinicals:
- Orchitis – inflammation of testis
- Hydrocele – excess fluid in TV
- Hematocele – blood in TV
- Varicocele – venous plexus dilated
- Spermatocele – collection of fluid in epididymis
- Vasectomy – vas deferens ligated and cut
- Distention of scrotum – indirect hernia
Spermatic cord
Forms at deep inguinal ring, enters scrotum via superficial inguinal ring, ends at posterior border of testis
Coverings:
- External spermatic fascia (aponeurosis of external oblique)
- Cremasteric muscle and fascia (internal oblique)
- Internal spermatic fascia (transversalis fascia)
Contents:
- Vas deferens
- Lymph vessels
- Testicular artery
- Cremasteric vessels
- Deferential artery
- Genital nerve
Clinicals:
- Hydrocele of cord
- Torsion of spermatic cord – Surgical emergency, twists on itself, occludes testicular artery and venous drainage leading to necrosis
- Cremasteric reflex

Penis

Coverings:
- Skin – thin, dark, prepuce covers glans
- Deep fascia of penis – continuation of perineal fascia
- Tunica albuginea
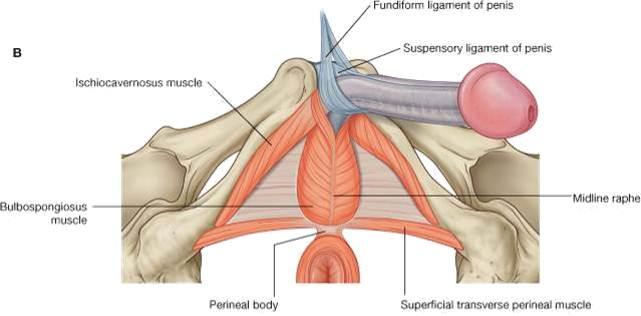
Support:
- Suspensory ligament – connects erectile bodies to pubic symphysis
- Fundiform ligament
Blood supply: Dorsal, deep and bulb of penis arteries
Venous:
- Deep dorsal vein – drains to prostatic venous plexus
- Superficial dorsal vein – drains to superficial external pudendal vein
Nerves:
- Paired dorsal nerve of penis (pudendal nerve) – sensory and sympathetic
- Cavernous nerves (prostatic nerve plexus) – parasympathetic, responsible for the vascular changes which cause erection
Lymphatics: Deep inguinal nodes (glans penis), superficial inguinal nodes
Clinicals:
- Hypospadias – Born with urethra opening on ventral aspect
- Circumcision – surgical excision of prepuce, glans exposed
- Impotence – inability to achieve erection
- Erectile dysfunction – inability to maintain erection
- Priapism – Persistent erection, blood trapped in erectile tissue, can lead to scarring or erectile dysfunction
Prostate gland
Position: Surrounds prostatic urethra, inferior to bladder neck
Relations:
- Anterior – Pubic symphysis
- Posterior – Ampulla of rectum
- Superior – Neck of bladder
- Inferior – External urethral sphincter
- Inferolateral – levator ani muscles
Blood supply: Prostatic artery (from internal iliac), middle rectal, internal pudendal
Venous: Prostatic venous plexus – drains to internal iliac veins
Nerves: Inferior hypogastric plexus
Lymphatics: Internal iliac, sacral nodes
Clinicals:
- Benign prostatic hyperplasia – enlargement of prostate with no malignancy, urinary frequency increases as it compresses bladder and urethra
- Cancer – spread via blood and lymph to IVC, vertebral column and pelvis
Seminal vesicle
Vas deferens combines with seminal vesicle duct to form ejaculatory duct which drains into prostatic urethra
Position: Between bladder fundus and rectum/rectovesical pouch
Relations:
- Anterior – Bladder fundus, ureter
- Posterior – Rectum
- Inferior – Prostate and ejaculatory duct
- Medial – Vas deferens
- Lateral – Prostatic venous plexus
Blood supply: Inferior vesicle, middle rectal, internal pudendal
Nerves: Inferior hypogastric plexus
Lymphatics: External and internal iliac lymph nodes
Clinicals: Seminal gland abscess – may rupture, pus enters peritoneal cavity
Vas deferens
Continuation of epididymis in spermatic cord
Course:
- From tail of epididymis
- Ascends posterior to testis
- Through spermatic cord
- Penetrate abdominal wall via inguinal canal
- Crosses external iliac vessels
- Turns medial between bladder and urethra
- Joins duct of seminal vesicle to form ejaculatory duct
Blood supply: Deferential artery
Venous: Testicular vein, prostate venous plexus
Lymphatics: External iliac
Clinicals: Vasectomy – male sterilization
These are summarized notes from various sources, mainly TeachMeAnatomy and Wikipedia
Perineum: Male and Female
Inferior part of pelvic outlet between thighs, separated from pelvic cavity superiorly by pelvic floor
Boundaries:
- Anterior – Pubic symphysis, mons pubis/base of penis
- Posterior – Tip of coccyx, intergluteal cleft
- Lateral – Medial thigh, inferior ischiopubic rami, sacrotuberous ligament
- Roof – Pelvic floor
- Base – skin and fascia

Blood supply: Internal and external pudendal
Nerves: Pudendal, ilioinguinal, posterior cutaneous nerve of thigh
Lymphatics:
- Glans penis/clitoris – Deep inguinal nodes
- Testis/ovaries – Lumbar
- Rest of perineum – Superficial inguinal
Perineal body:
Fibromuscular mask at junction of urogenital and anal triangle. Has skeletal muscles, smooth muscles, collagen and elastic fibers
Muscles that attach to it:
- Levator ani
- Bulbospongiosum
- Superficial and deep transverse perineal muscles
- External anal sphincter
- External urethral sphincter
Clinicals:
- Damage during childbirth – Stretching or tearing, therefore possible prolapse of pelvic viscera. Can be avoided by episiotomy (surgical cut in the muscular area between the vagina and the anus)
- Pudendal and ilioinguinal nerve block – during labour or episiotomy
Anal triangle
Contents:
- Anal aperture
- External anal sphincter muscle
- Two ischioanal fossae – spaces lateral to anus
Ischioanal/ischiorectal fossae:
Boundaries:
- Anterior – Pelvic diaphragm, perineal body
- Posterior – Sacrotuberous ligament, gluteus maximus
- Superior – Levator ani
- Inferior – Perineal skin
- Medial – Anal canal, external sphincter
- Lateral – Ischial tuberosity, obturator internus
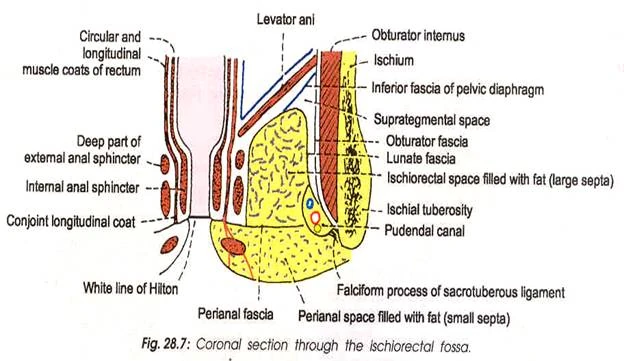
Content:
- Fat
- Internal pudendal vessels
- Pudendal nerve
- Inferior rectal vessels and nerve
Clinicals:
- Ischianal abscess – infection due to wound
- Anal fissure – anal valve tears
Urogenital triangle
Coronal section:

Superficial perineal pouch:
Boundaries:
- Anterior – continuous with Scarpa’s fascia
- Roof – Perineal membrane
- Floor – Perineal fascia
- Lateral – Ischiopubic ramus
Contents:
- Root of penis
- Superficial perineal muscles
- Ischiocavernosus and bulbospongiosum muscles
- Vestibular glands (♀)
- Superficial transverse perineal nerve
- Clitoris (♀)
- Bulb of vestibule (♀)
Deep perineal pouch:
Boundaries:
- Superior – Pelvic diaphragm
- Inferior – Perineal membrane
- Lateral – Obturator fascia
Contents:
- Deep transverse perineal muscles
- External urethral sphincter
- Membranous urethra
- Bulbourethral glands
- Internal pudendal vessels
- Artery of bulb of penis
Clinicals:
- Extravasation of urine – interruption of urethra, collection of urine in scrotum or penis
- Bartholin’s gland cyst
Pelvic diaphragm
Separates pelvic cavity (true pelvis) and perineum (genitalia and anus)
Pelvic viscera (bladder, rectum, genital organs) reside in pelvic cavity
Pierced by: Rectal hiatus, urogenital hiatus (urethra, vagina)
Functions:
- Support viscera
- Resistance to increase in intrapelvic pressure while coughing etc
- Sphincter action on urethra and rectum
- Support fetal head
Clinicals:
- Injury during childbirth – prolapse of pelvic viscera, urinary/rectal incontinence
Urinary bladder
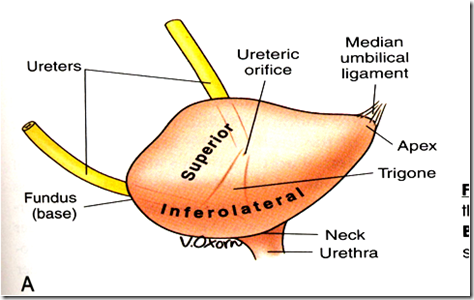
Position: Anterior in pelvic cavity, posterior to pubic symphysis, infront of uterus, cervix and vagina
2 sphincters:
1. Internal urethral sphincter:
- Males: Circular smooth fibers, autonomic control, prevent seminal regurgitation during ejaculation
- Females: No muscle
2. External urethral sphincter: Skeletal muscle under voluntary control
Relations:
- Anterior – pubic bone, median umbilical ligament
- Posterior – Rectum, vas deferens, seminal vesicle, vagina, uterus
- Superior – Peritoneum, sigmoid colon, coils of small intestine, fundus of uterus
- Inferior – Pelvic diaphragm, prostate
- Lateral – Obturator internus, levator ani muscles
Support: Median umbilical ligament, pelvic diaphragm, urogenital diaphragm, puboprostatic ligament (males) and pubovesical ligament (females)
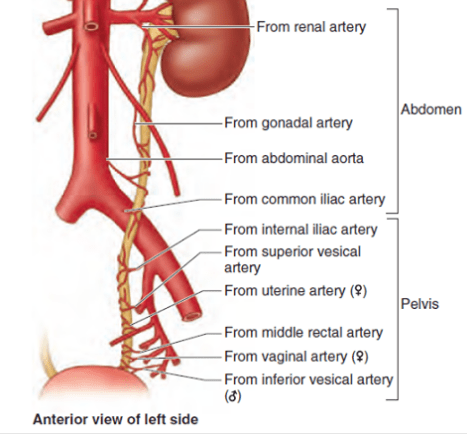
Blood supply: Superior and inferior vesical, obturator, inferior gluteal, vaginal and uterine (for females)
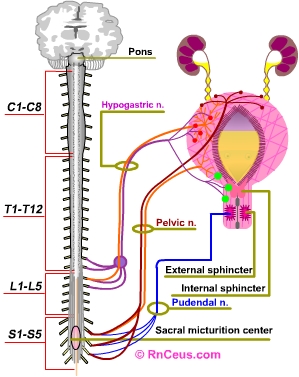
Nerves:
- Sympathetic – Hypogastric nerve (T12-L2) – relax detrusor muscle, urine retention
- Parasympathetic – Pelvic splanchnic (S2-S4) – contract detrusor muscle, stimulate micturition
- Somatic – Pudendal nerve (S2-S4) – innervate external urethral sphincter, constrict (storage), relax (micturition)
Lymphatics: Internal and external iliac
Bladder stretch reflex:

Clinicals:
- Spinal cord injury:
- Above T12 – No awareness of bladder filling, no control over external sphincter, constantly relaxed bladder
- Below T12 – Flaccid bladder, detrusor muscle paralysed, bladder fills uncontrollably
- Rupture of bladder – fracture/injury, urine escapes to extraperitoneal or intraperitoneal
- Cystocele – prolapsed bladder into anterior vagina wall
- Cystostomy – opening of bladder to drain urine
- Cystoscopy camera inserted into bladder via urethra
Urethra
Extent:
- Males: Internal urethral orifice (bladder) – external urethral orifice (tip of glans)
- Females: Neck of bladder – urethral orifice in vetibule
Blood supply: Inferior vesical, middle rectal, dorsal artery of penis, artery of bulb, internal pudendal, vaginal
Venous: Prostatic venous plexus, internal pudendal
Nerves: Inferior hypogastric plexus (sympathetic and parasympathetic), pudendal (somatic)
Lymphatics: Internal iliac, deep inguinal
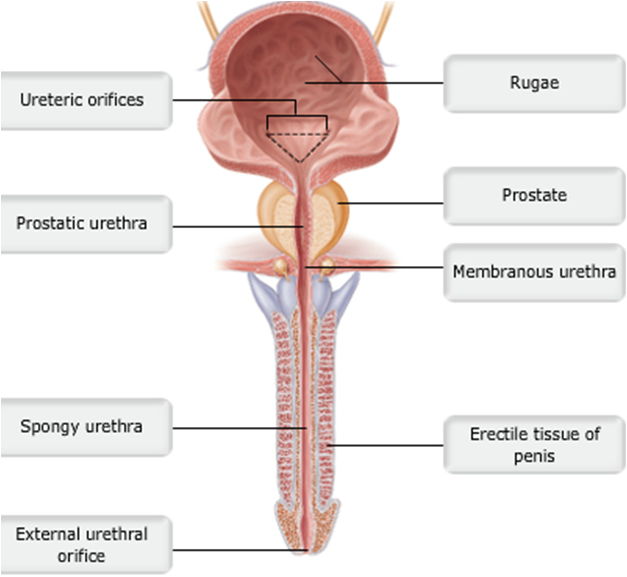
NB: Male urethra divided into 4 parts:
- Preprostatic: Internal urethral orifice – prostrate
- Prostatic: Through prostate gland, ejaculatory duct and prostatic ducts drain into urethra here
- Membranous: Surrounded by external urethral sphincter – voluntary control
- Spongy: Through bulb and corpus spongiosum, bulbourethral glands empty here
Clinicals:
- Urinary tract infection
- Male catheterisation – insert tube through urethra into bladder when patient cannot pass urine
Rectum
Position: True pelvis, posterior end
Flexures: 2 anteroposterior and 3 lateral
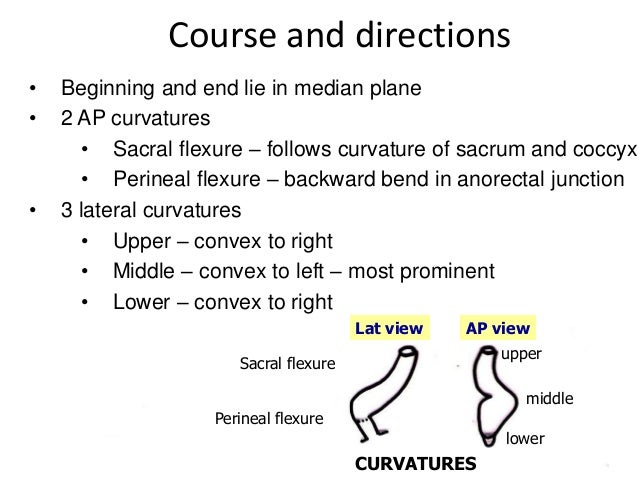
Final segment of rectum is called ampulla – relaxes to store faeces
Relations:

Blood supply:
- Superior rectal (from IMA)
- Middle rectal (from internal iliac)
- Inferior rectal (from internal pudendal)
Nerves: Hypogastric plexus
Lymphatics: Pararectal and internal iliac
Clinicals:
- Hemorrhoids – thrombosis of external rectal plexus
- Proctoscope – examine anal canal, rectum and sigmoid colon
- Rectocele
- Digital rectal examination
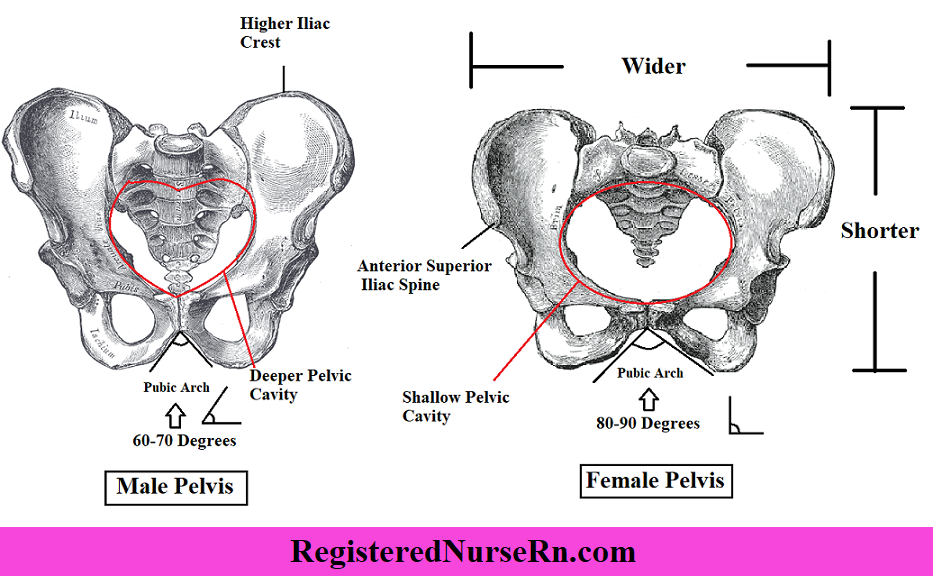
Difference between male and female pelvis
Anal canal
Position: In anal triangle between ischioanal fossae, from rectum to anus
Relations:
- Lateral: Ischioanal fossae
- Posterior: Coccyx and sacrum
- Anterior: Perineal body, urogenital diaphragm, urethra, bulb of penis, vagina
Sphincters:
- Internal – upper 2/3, involuntary
- External – Lower 1/3, voluntary
NB: Pectinate line – divides anal canal into upper (embryonic hindgut) and lower (ectoderm of proctodeum) parts
Blood supply: Superior rectal (above pectinate line), Inferior rectal (below)
Nerves: Autonomic – Inferior hypogastric plexus (above pectinate line), Somatic – pudendal nerve (below)
Lymphatics: Internal iliac (above pectinate line), superficial inguinal (below)
Clinicals:
- Anal fissure – anal valve tears
- Hemorrhoids – constipation
- Perianal abscess
- Anal fistula
- Anorectal incontinence – pudendal nerve damage
These are summarized notes from various sources, mainly TeachMeAnatomy and Wikipedia
Anatomy of Abdomen
Arteries

(I) Abdominal aorta:
- Lower border of T12 – lower border of L4 (aortic hiatus to bifurcation)
- Travels down posterior wall of abdomen
- Runs on the left and parallel to IVC
- At L4 bifurcates
Relations:
- Anterior – Lesser omentum, stomach, pancreas
- Posterior – Vertebral column, lumbar veins
- Right – IVC, azygos vein, cisterna chyli, right crus diaphragm
- Left – Left crus diaphragm, ascending duodenum, small intestines
Clinicals:
- Rupture of abdominal aortic aneurysm – deep pain in abdomen, back pain, hemoperitoneum (blood in peritoneal cavity) – leads to hemorrhagic shock – rapid death
(II) Celiac trunk:
- 1st branch of abdominal aorta – T12
- Divides into 3 branches
(III) Superior mesenteric artery:
- 2nd branch of abdominal aorta – L1
- Posterior to neck of pancreas
- Pass between pancreas head and uncinate process
- Terminates in right iliac fossa as ileocolic artery
(IV) Inferior mesenteric artery:
- 3rd branch of abdominal aorta – L3
- Posterior to left psoas major
- Terminates as superior rectal artery
Clinicals:
- Peptic ulcers – erode gastroduodenal artery, leads to gastrointestinal bleeding
- Celiac trunk compression syndrome – due to median arcuate ligament, leads to ischemia (median arcuate ligament connects right and left crura of diaphragm)
- Splenic artery aneurysm
- Left hemicolectomy – surgical removal of descending colon – dissect branches of IMA and IMV
Veins

(I) IVC:
- Formed by left and right common iliac veins at L5
- Ascends on right of vertebral column and aorta
- Anterior to right psoas major
- Grooves liver
- Enters through diaphragm at T8 – caval opening
Relations:
- Anterior – Head of pancreas, epiploic foramen, right and caudate lobe liver
- Posterior – Right psoas major, right crus diaphragm, Lower lumbar vertebrae
- Right – Right kidney, right lobe liver
- Left – Abdominal aorta
(II) IVC and SVC communication sites:
1. Thoracoepigastric – connects lateral thoracic vein (axillary vein – SVC) and superficial epigastric vein (femoral vein – IVC)
2. Superior epigastric (internal thoracic – SVC) and inferior epigastric (external iliac – IVC)
3. Azygos venous system
4. Vertebral venous plexus – Lumbar veins (IVC) and posterior intercostal veins (SVC)
(III) Portal vein:
- Formed from superior mesenteric vein and splenic vein – behind neck of pancreas
- Before reaching liver, portal vein divides into right and left branches – divides in to smaller venous branches
- Drains into hepatic sinusoids (supply blood to liver)
Clinicals:
- Portal hypertention – obstruction of blood flow through portal system, blood redirected through portosystematic anastomosis, veins become dilated – varices and hemorrhoids
- Infection of portal vein (pylephlebitis)
Nerves
(I) Nerves of abdominal wall: Somatic – Parietal peritoneum and skin
1. Anterolateral abdominal wall: Anterior rami of:
- T7-T9 – Skin superior to umbilicus
- T10 – Skin around umbilicus
- T11 – Skin inferior to umbilicus
- T12/Subcostal – Skin inferior to umbilicus
- L1 – Iliohypogastric and ilioinguinal – Skin inferior to umbilicus
2. Posterior abdominal wall:
- T12 – subcostal
- Lumbar (L1-L5): Iliohypogastric and ilioinguinal (L1), Gentitofemoral (L1-L2), Lateral cutaneous femoral (L2-L3), Femoral (L2-L4), Obturator (L2-L4), Lumbosacral trunk (L4-L5)

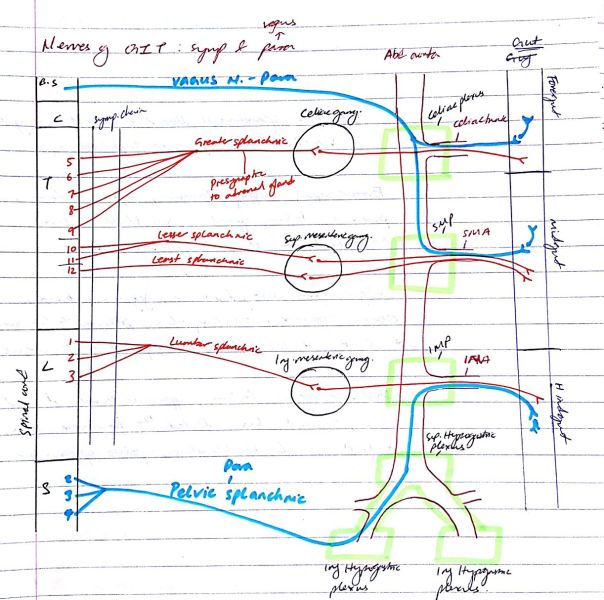
(II) Nerves of GIT: Visceral – Abdominal viscera and visceral peritoneum
Sympathetic: vasoconstrict blood vessels, decrease peristalsis and digestion, close sphincters of GIT
Parasympathetic: vasodilate blood vessels, increase peristalsis and digestion, stimulate insulin production
NB:
- If a sympathetic nerve is supplying a thoracic viscera – Synapse occurs in sympathetic chain
- If a sympathetic nerve is supplying an abdominal viscera – No synapse, but passes through the chain and synapses at the celiac ganglion, SMG or IMG
1. Presynaptic fibers T5-T9 ⇒ Greater splanchnic nerve – Sympathetic
- Synapse in celiac ganglion
- Post synaptic fibers – pass in celiac plexus – towards branches of celiac trunk and supplies foregut organs
2. Presynaptic fibers T10-T11 ⇒ Lesser splanchnic nerve – Sympathetic
- Synapse in SMG
- Post synaptic fibers – pass in SM plexus – towards branches of SMA and supplies midgut organs
3. Presynaptic fibers T12 ⇒ Least splanchnic nerve – Sympathetic
- Synapse in SMG
- Post synaptic fibers – pass in SM plexus – towards branches of SMA and supplies midgut organs
4. Presynaptic fibers L1-L3 ⇒ Lumbar splanchnic nerve – Sympathetic
- Synapse in IMG
- Post synaptic fibers – pass in IM plexus – towards branches of IMA and supplies hindgut organs
5. Vagus nerve – Parasympathetic
- Presynaptic fibers of vagus – through celiac plexus – synapses at small ganglion of the foregut organ
- Presynaptic fibers of vagus – through SM plexus – synapses at small ganglion of the midgut organ
6. Presynaptic S2,S3,S4 – Pelvic splanchnic nerve – Parasympathetic
- Run in inferior hypogastric plexus – ascend to superior hypogastric plexus – then to inferior mesenteric plexus – along branches of IMA
- Synapse at small ganglion of hindgut organ
Blood and nerve supply of foregut, midgut and hindgut organs
Foregut organs: Esophagus, stomach, 1st part duodenum, pancreas, liver, gallbladder
- Artery – Celiac trunk
- Nerve – Greater splanchnic, vagus
Midgut organs: Rest of duodenum, jejunum, ilium, cecum, appendix, ascending colon, proximal 2/3 transverse colon
- Artery – SMA
- Nerve – Lesser splanchnic, least splanchnic and vagus
Hindgut organs: Rectum, upper anal canal, descending colon, sigmoid colon, distal 1/3 transverse colon
- Artery – IMA
- Nerve – Lumbar splanchnic, pelvic splanchnic
Abdomen
Longitudinal section of abdomen:

Supracolic and infracolic connected by paracolic gutters – drain fluid such as pus or bile to outer margins of colon (Clinical – spread infection, tumor deposits from or to pelvis)

Organs are covered by visceral peritoneum. Between parietal and visceral peritoneum is peritoneal fluid (contains electrolytes, antibodies, WBC, glucose)
Clinical: Ascites – fluid accumulation
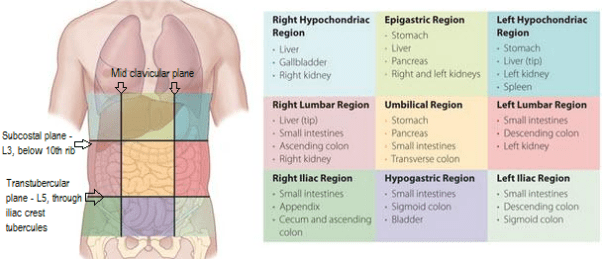
Regions of abdomen:
Clinicals:
- Pain location, surgical procedures
- Abdominal hernias:
- Internal – hiatus of diaphragm, epiploic foramen
- External – inguinal, femoral, obturator
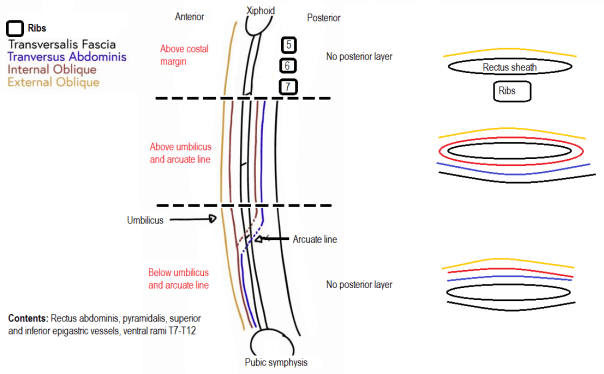
Anterior abdominal wall
Layers:
- Skin
- Superficial fascia:
- Above umbilicus – single sheet of connective tissue
- Below umbilicus – fatty Camper’s fascia then membranous Scarpe’s fascia
- Muscles: enclosed in deep investing fascia
- External oblique
- Internal oblique
- Transverse abdominis
- Fascia transversalis
- Extraperitoneal fatty areolar tissue
- Parietal peritoneum
NB:
- In the centre is rectus muscle
- Scarpe’s fascia continues as Colle’s and Darto’s fascia and is inferiorly attached to fascia lata below inguinal ligament. Therefore when penile urethra injured in men, urine escapes urethra to scrotum and spreads in lower abdominal wall but not to thigh.
Functions:
- Contain and protect abdominal contents
- Increase intraabdominal pressure in micturition, defecation, coughing, sneezing and parturition
- Cause trunkal flexion
- Contribute to venous return
Blood supply:
- Internal thoracic – Superior epigastric, musculophrenic
- Abdominal aorta – Posterior intercostal, subcostal
- External iliac – Inferior epigastric, deep circumflex iliac
- Femoral – Superficial circumflex iliac, superficial epigastric
Nerves: Written in nerves
Lymph:
- Superficial:
- Superior to umbilicus – Anterior axillary and parasternal
- Inferior to umbilicus – Superficial inguinal
- Deep: External iliac, lumbar nodes
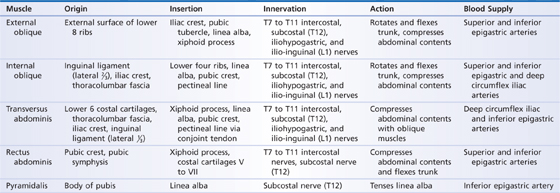
Anterior Abdominal wall muscles:
Clinicals:
- Abdominal incision/ Laparotomy – most common is midline incision along linea alba from xiphoid process to umbilicus to pubic symphysis
- Urinary extravasation – penile urethra injured in men, urine escapes urethra to scrotum and spreads in lower abdominal wall but not to thigh
- Venous engorgement – flow in SVC or IVC obstructed, leads to collateral flow
- Ascites
- Caput medusae – engorged superficial epigastric veins
- Liposuction
Rectus sheath
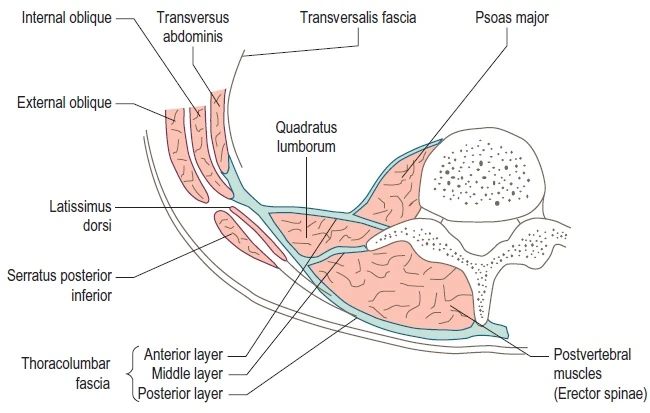
Posterior abdominal wall
Fascia:
- Fascia transversalis
- Psoas major fascia
- Thoracolumbar fascia – 3 layers
Clinicals:
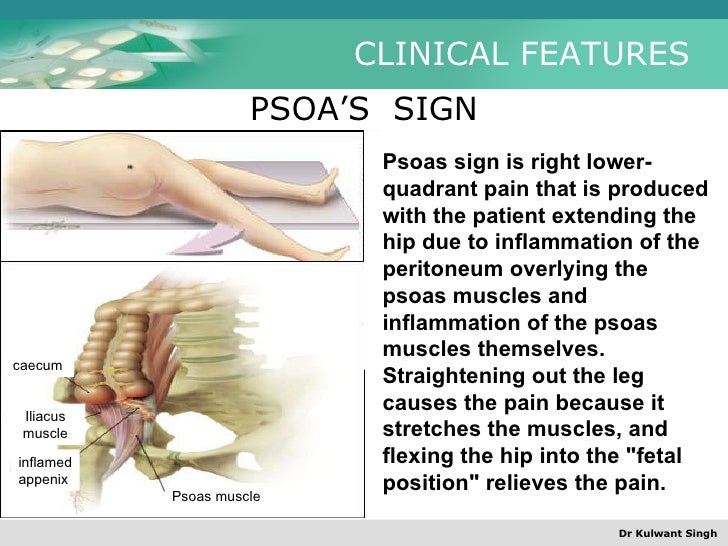
- Psoas abscess – caused by lumbar tuberculosis, infects psoas sheath
- Psoas sign
Inguinal canal
Superior and parallel to inguinal ligament

Boundaries:
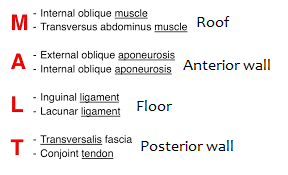
Contents: Ilioinguinal nerve, genitofemoral nerve, round ligament (females), spermatic cord (males)
Inguinal triangle of Hesselbach

Clinicals:

Peritoneum
Closed sac except in females where infundibulum opens
Layers: Parietal and visceral
Intraperitoneal organs: Stomach, spleen, liver, transverse colon
Retroperitoneal organs: Primary (retro since developed – KER) and secondary (become retro later – SADPUC)
Retroperitoneal viscera:
- S – Suprarenal glands
- A – Aorta and IVC
- D – Duodenum (2nd part)
- P – Pancreas
- U – Ureter
- C – Colon (ascending and descending)
- K – Kidney
- E – Esophagus
- R – Rectum
Ligaments:
- Median umbilical ligament (allantoic duct) – urinary bladder apex to umbilicus
- 2 medial umbilical ligaments (umbilical arteries)
- 2 lateral umbilical ligaments – cover inferior epigastric artery
NB: Umbilical vein – becomes ligamentum teres of liver
Mesenteries: Fold of visceral peritoneum that attatches intraperitoneal organs to posterior abdominal wall. Contains nerves, vessels, lymph nodes and fat
Omenta:
- Greater omentum – From greater curvature stomach and proximal duodenum ⇒ to infront of small intestines ⇒ Reflects and ascends to transverse colon

Contains: Nerves, vessels, lymph nodes and fat
Parts: Gastrosplenic ligament, gastrophrenic ligament, gastrocolic ligament
Functions:
- Infection and wound isolation
- Limit spread of intraperitoneal infections
- Immunity – macrophages, lymphocytes etc
- Mobility
- Insulation
2. Lesser omentum – From lesser curvature stomach to liver
Parts: Hepatogastric ligament (right and left gastric arteries), hepatoduodenal ligament (Common bile duct, portal vein, hepatic artery)
Peritoneal cavity:
Epiploic foramen – Relations:
- Superior – Caudate lobe liver
- Inferior – 1st part duodenum
- Anterior – Hepatoduodenal ligament
- Posterior – IVC
Clinicals:
- Internal hernia
- Accumulation of blood (ruptured spleen), bile (bile duct) or fecal matter (intestines)
- Peritonitis – infection due to bacterial contamination
Liver
Ligaments:

Impressions on liver:
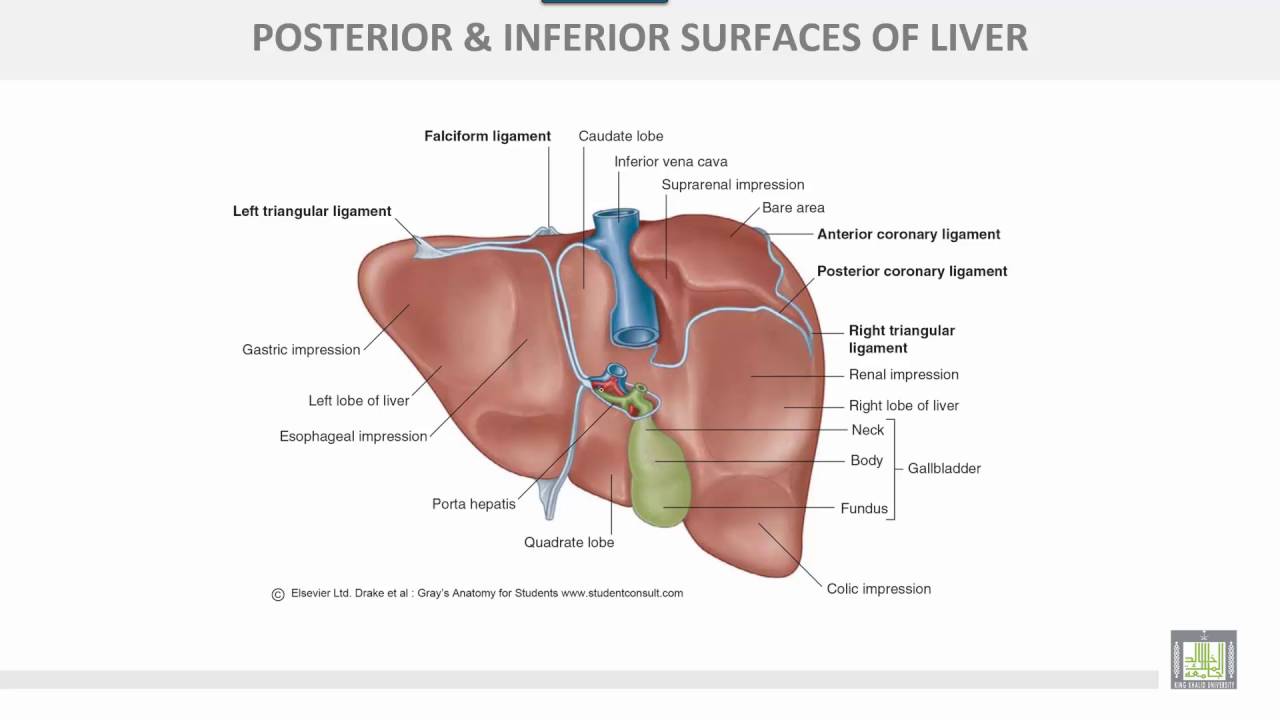
Position: Right 1/4, deep to ribs 7-11
Surfaces: Diaphragmatic and visceral
Relations:
- Anterior: Diaphragm, ribcage, falciform ligament
- Posterior: Right kidney and adrenal, gall bladder, esophagus, stomach
- Superior: Diaphragm
- Inferior: Gall bladder
Support structures: Falciform ligament, coronary ligament, ligamentum teres, triangular ligament, hepatoduodenal ligament, lesser omentum and hepatic veins
Blood supply: Right and left hepatic arteries – segmental branches
Venous: Hepatic portal vein – drains to hepatic sinusoids and so to IVC
Nerves: Sympathetic – Greater splanchnic, Parasympathetic – Vagus, right phrenic
Lymphatics: Hepatic, left gastric nodes
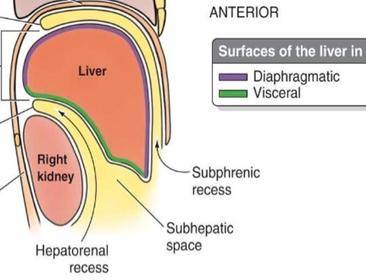
Hepatic recesses:
- Right and left subphrenic spaces – between diaphragm and liver
- Subhepatic space – between inferior surface liver and transverse colon
- Morrison’s pouch/ hepatorenal – between liver and right kidney
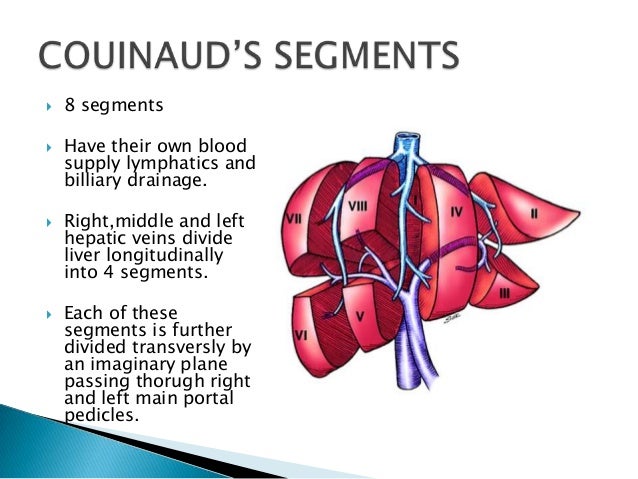
Functional divisions of liver:
Clinicals:
- Hepatic lobectomies
- Rupture of liver – fractured rib, hemorrhage
- Liver trauma – tearing of hepatic veins from IVC
- Hepatomegaly – enlarged liver – due to infection, tumours or metabolic disorder
- Liver cirrhosis – health tissue replaced by scar tissue, organ will start to fail, blood cannot easily flow in portal vein
- Liver biopsy – small needle inserted in liver to collect tissue sample
- Jaundice
Gallbladder
Location: Between right and left lobes, inferior surface of liver
Biliary tree:

Relations:
- Anterior – Inferior surface liver
- Posterior – Transverse colon, proximal duodenum
- Superior – Liver
- Inferior – Biliary tree
Blood: Cystic artery
Venous: Cystic vein, hepatic sinusoids
Nerves: Sympathetic – Greater splanchnic, Parasympathetic – Vagus, right phrenic
Lymph: Hepatic nodes
Clinicals:
- Mobile gallbladder – only attached to cystic duct, risk of torsion
- Cholecystectomy
- Gall stones
- Biliary colic – gall stones block bile duct
- Cholecystitis – inflammation
Spleen
Impressions:

Surfaces: Diaphragmatic and visceral
Relations:
- Anterior: Stomach
- Posterior: Left kidney and adrenal, ribs 9-11
- Inferior: Left colic flexure
Support structures:
- Gastrosplenic ligament (short gastric vessels) – great curvature to spleen
- Splenorenal ligament (Splenic vessels) – spleen to left kidney
- Phrenicocolic ligament – diaphragm to left colic flexure
Blood supply: Splenic artery – 5 segmental arteries
Venous: Splenic vein
Nerves: Sympathetic – Greater splanchnic, Parasympathetic – Vagus, right phrenic
Lymphatics: Celiac nodes
Clinicals:
- Rupture of spleen – fractured rib, intraperitoneal hemorrhage
- Splenectomy
- Splenomegaly
- Accessory spleen
- Splenic biopsy
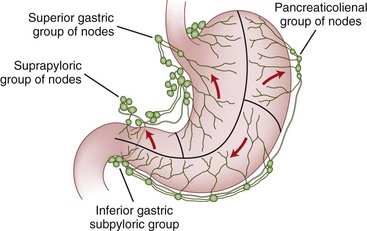
Stomach

Relations:
- Anterior – Left lobe liver
- Posterior – Lesser sac, spleen, left kidney and adrenal, splenic artery, pancreas, aorta
- Inferior – Transverse colon, left colic flexure
Blood supply:

Nerves: Sympathetic – Greater splanchnic, Parasympathetic – Vagus, right phrenic
Lymphatics:
Clinicals:
- Esophageal varices – portal hypertension
- Pyrosis (heart burn) – due to gastroesophageal reflex disorder (stomach acid flows to esophagus)
- Gastroesophageal reflex disorder – hiatus hernia, delayed gastric emptying, dysfunction of lower esophagus sphincter
- Hiatus hernia – part of stomach protrudes through esophageal hiatus in diaphragm
- Pylorospasm – closure of pylorus due to muscle spasm, due to pyloric ulcers
- Gastrectomy
- Gastric ulcers – erode arteries nearby
Pancreas
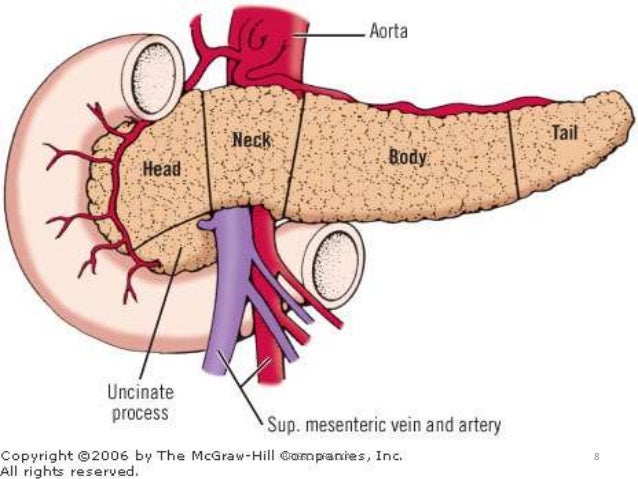
Relations:
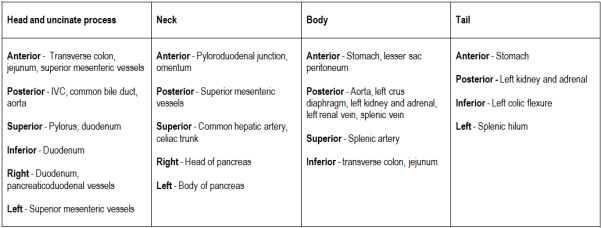
Blood supply: Greater pancreatic artery (from splenic artery), Superior and inferior pancreaticoduodenal artery
Nerves: Sympathetic – Greater splanchnic, Parasympathetic – Vagus, right phrenic
Lymphatics: Pancreaticosplenic, pancreaticoduodenal
Clinicals:
- Blocked hepatopancreatic ampulla – gallstone
- Pancreatitis
- Pancreatic ectomy
- Rupture
- Cancer
Duodenum
From pylorus to duodenojejunal junction

Relations:
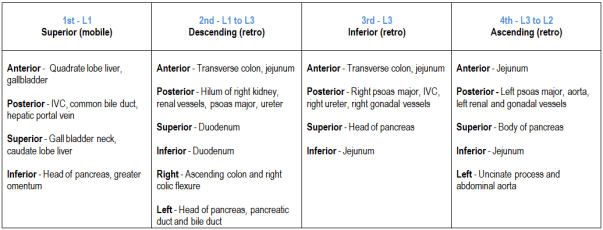
Support structures: Hepatoduodenal ligament, ligament of Trietz
Recesses:

Blood supply: Superior and inferior pancreaticoduodenal, right gastroepiploic
Nerve: Sympathetic – Greater and lesser splanchnic, Parasympathetic – Vagus
Lymphatics: Pancreaticoduodenal nodes, superior mesenteric nodes
Clinicals:
- Duodenal ulcers – erode gastroduodenal artery – hemorrhage
- Paraduodenal hernia – intestinal loops
Jejunum and ileum
From duodenojejunal junction to ileocecal junction

Blood supply: SMA and vasa recta
Nerves: Lesser splanchnic, least splanchnic and vagus
Clinicals: Ischemia of intestine – occlusion of vasa recta by embolus
Large intestine
From ileocecal valve in right iliac fossa to anal orifice

NB: Ascending colon has no mesentary
Relations:
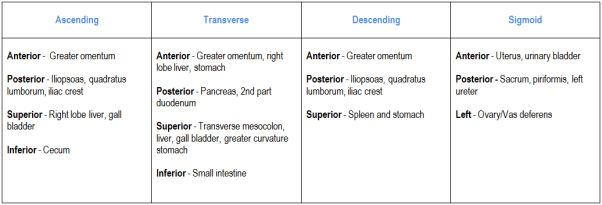
Blood supply:

Nerves:
- Lesser splanchnic, least splanchnic and vagus – Cecum, appendix, ascending colon, proximal 2/3 transverse colon
- Lumbar splanchnic and pelvic splanchnic – Distal 1/3 transverse, descending and sigmoid coloc
Lymphatics: Epicolic and paracolicdrain into superior and inferior mesenteric nodes
Clinicals:
- Colitis
- Colectomy
- Ileostomy – artificial opening of ileum through abdominal wall
- Colonoscopy
- Diverticula – pouches form on wall of colon (usually sigmoid) – old people
- Volvulus sigmoid- sigmoid colon twists on sigmoid mesocolon – bowel obstruction
Difference between small and large intestine:

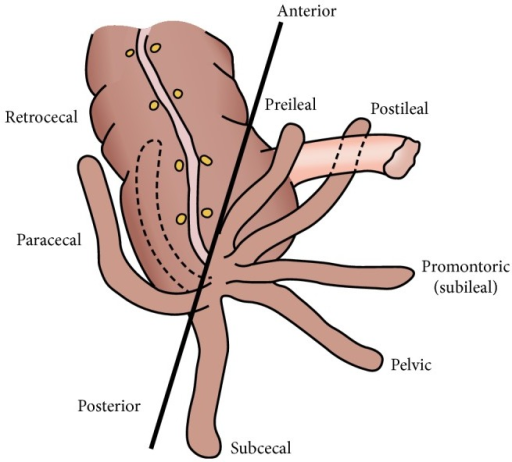
Appendix
Location: Right iliac fossa, opens in cecum
Relations:
- Anterior – Greater omentum
- Posterior – Psoas major
- Superior – Ileum, mesoappendix (portion of the mesentery connecting the ileum to the appendix)
- Left – Sigmoid colon
- Right – Paracolic gutter, ascending colon
Positions:
Blood supply: Appendicular artery and vein
Nerves: Lesser splanchnic, least splanchnic and vagus
Lymphatics: Superior mesenteric
Clinicals:
- Appendicitis
- Appendectomy
- Psoas test
Kidneys
Are 3 vertebrae long
Coverings: Superficial to deep
Pararenal fat ⇒ Renal fascia (enclose kidney and suprarenal glands) ⇒ Perirenal fat ⇒ Fibrous renal capsule
Support structures: Splenorenal ligament
Relations:
Anterior:
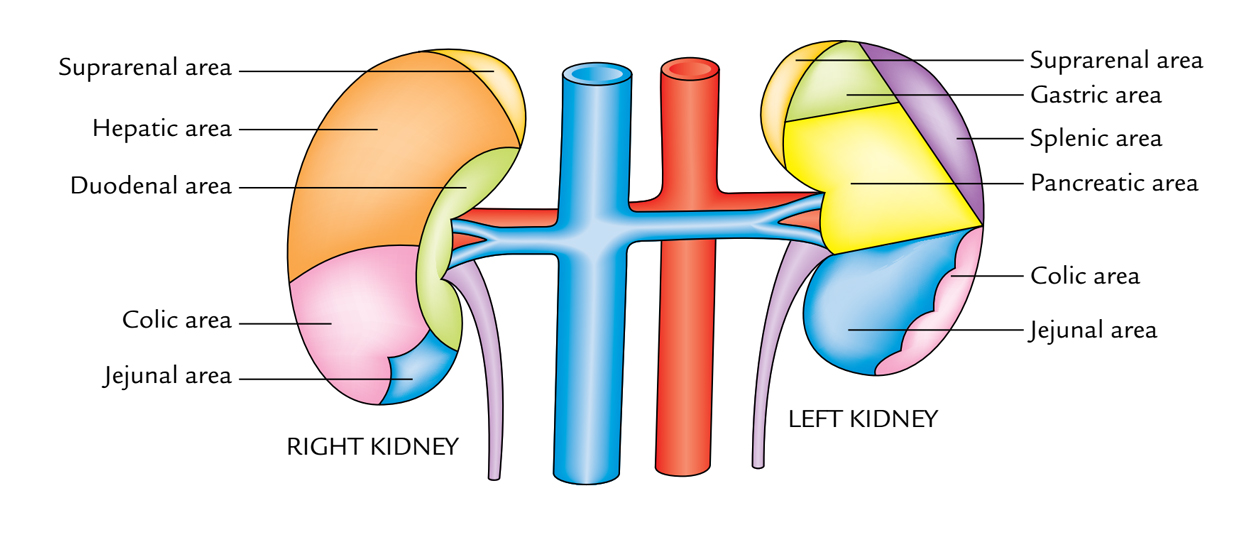
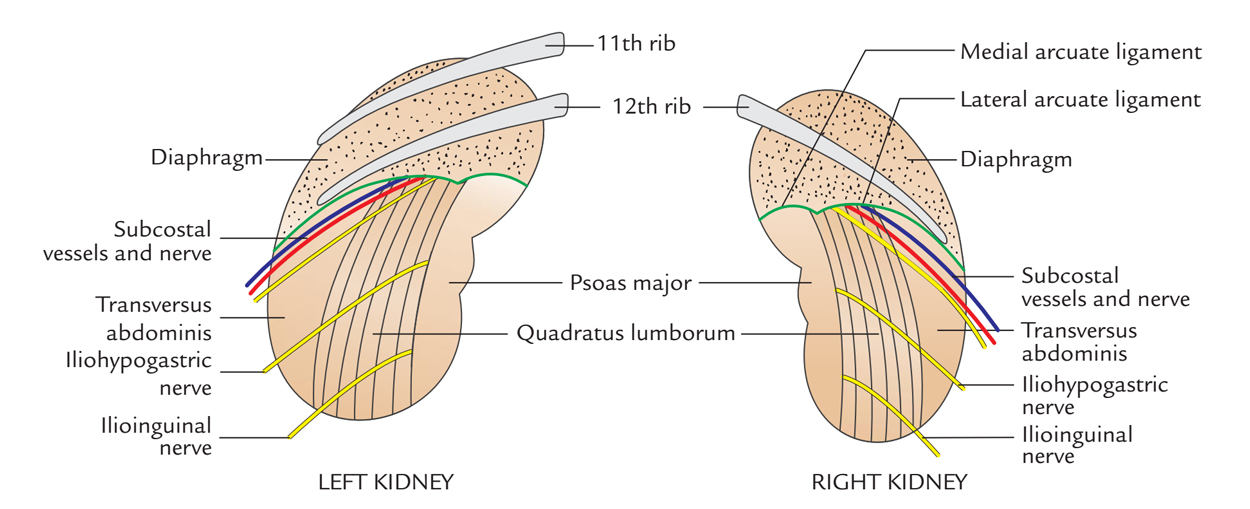
Posterior:
Blood supply:

Nerves: Lesser splanchnic, least splanchnic and vagus
Lymphatics: Lumbar nodes
Clinicals:
- Perinephric abscess – pus around kidney
- Pelvic kidney
- Horseshoe kidney
- Renal agenesis
- Renal hypoplasia
- Kidney stones/renal calculi – formed in kidney or renal pelvis, may pass through ureter into bladder
- Renal transplant – to lower abdomen, renal vessels connected to recipient external iliac vessels, ureter sutured into urinary bladder
- Nephrectomy
- Floating kidney – abnormal condition in which the kidney drops down into the pelvis when the patient stands up
Suprarenal glands
Cortex (mesoderm) and medulla (ectoderm – neural crest). Fatty tissue between kidney and suprarenal gland, covered in renal fascia.
Relations:
Right:
- Anterior – Right lobe liver
- Posterior – Right crus diaphragm
- Superior – Liver
Left:
- Anterior – Stomach, pancreas, spleen
- Posterior – Left crus diaphragm
- Superior – Spleen
Blood supply: Superior, middle and inferior suprarenal
Venous: Right and left suprarenal
Nerves: Greater splanchnic, lesser splanchnic
Lymphatics: Lumbar nodes
Right and left difference:
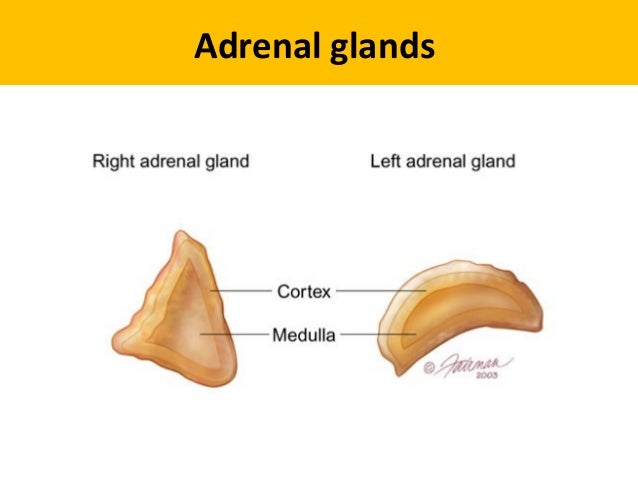
Right – Triangular shape, loosely attached to superior pole kidney
Left – Cresent shape, superior and middle border can extend to renal hilum
Clinicals:
- Tumor of medulla
- Addison’s disease – low cortisol and aldosterone
- Cushing’s syndrome – elevated cortisol
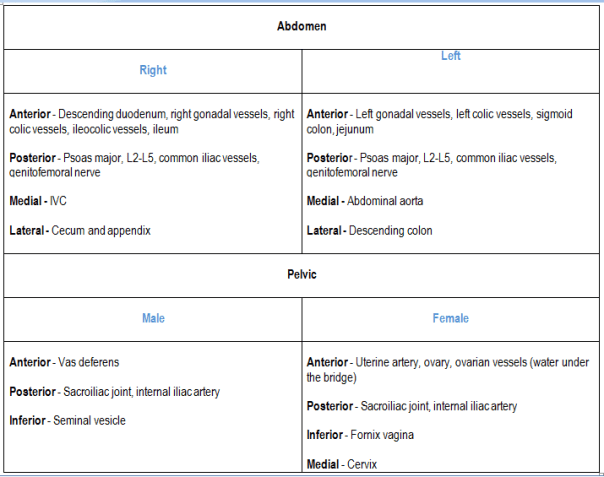
Ureter
Course:
- Continuation of renal pelvis
- Posterior to renal vessels
- Anterior to psoas major
- Gonadal vessels cross over it from medial to lateral
- Cross infront of common iliac bifurcation
- Opposite sacroiliac joint
- Opposite ischial spine, curves anteromedial to open into posterior superior part of bladder
- Runs an oblique 2cm course in urinary bladder wall – forms valve like mechanism
Blood supply:
Nerves: Renal plexus, superior hypogastric plexus, T11-L2
Lymphatics: Lumbar, common iliac, external iliac, internal iliac
Relations:
Clinicals:
- Retrocanal ureter – Right ureter passes posterior to IVC, disturbs drainage from right kidney
- Kidney stones – Obstruct urine flow
Others
1. Lumbar triangle:

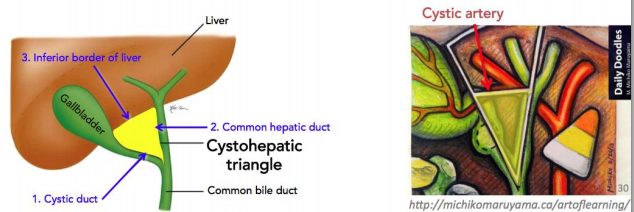
2. Calot’s triangle/Cystohepatic triangle:
Content: Cystic artery
3. Triangle of doom:
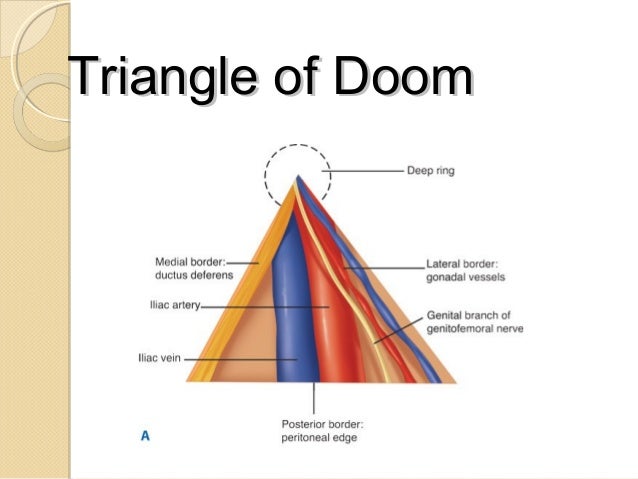
Contents:
- External iliac vessels
- Deep circumflex iliac vein
- Femoral nerve
- Genital branch of genitofemoral nerve
Clinicals: Inguinal hernia – nerves damaged when repairing a hernia by sutures or staples
4. Triangle of pain:

5. Triangle of safety:
For intercostal catheter placement

6. Modification of fascia transversalis:
- Femoral sheath and ring – anterior
- Deep inguinal ring – posterior
- Internal spermatic fascia in testis
7. Mcburney’s point:

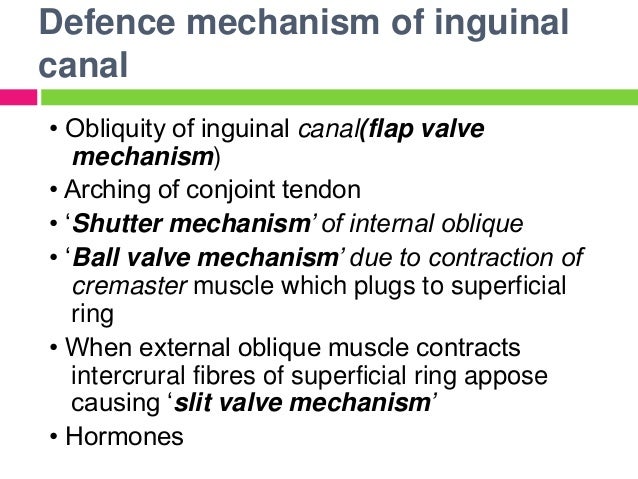
8. Mechanisms to prevent inguinal hernia:
These are summarized notes from various sources, mainly TeachMeAnatomy and Wikipedia
Anatomy of Thorax
Lung’s pleura
2 pleuras: continuous at hilum
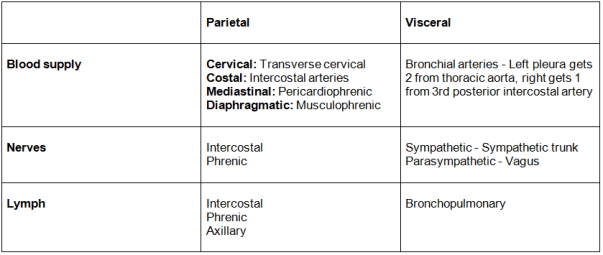
- Parietal pleura – lines inner surface of the thoracic cavity
- Visceral pleura – lines surface of lung
Pleural cavity: contains pleural fluid which lubricates lungs
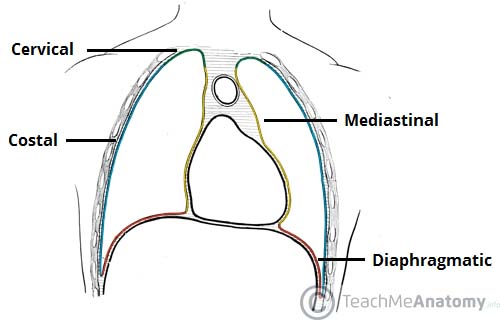
4 parts of parietal pleura:
Pleural recesses:

Clinicals:
- Drain fluid – insert needle superior to rib
- Pleuritis
- Pancoast tumor – on lung apex, erodes 1st rib
- Pyothorax (pus), hemothorax (blood), pneumothorax (air), chylothorax (lymph) – collect in pleural cavity
Lungs
Lung surfaces: Costal, mediastinal, diaphragmatic
Blood supply: Same as visceral pleura
Nerve: Same as visceral pleura
- Sympathetic trunk: Relax bronchial smooth muscle, vasoconstrict vessels
- Vagus: Contract smooth muscles, vasodilate
Bronchial tree: Trachea ⇒ Right and left bronchus ⇒ Lobar bronchus (3 right, 2 left) ⇒ Segmental bronchus ⇒ Interlobular bronchus ⇒ Terminal bronchiole ⇒ Respiratory bronchiole
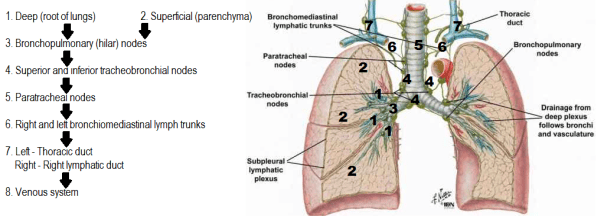
Lymphatics:
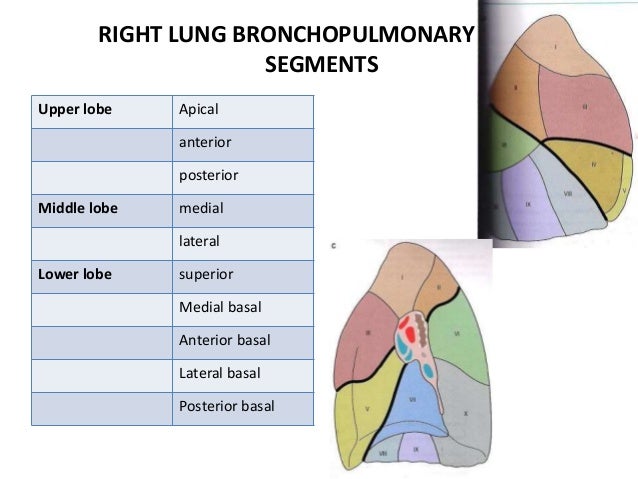
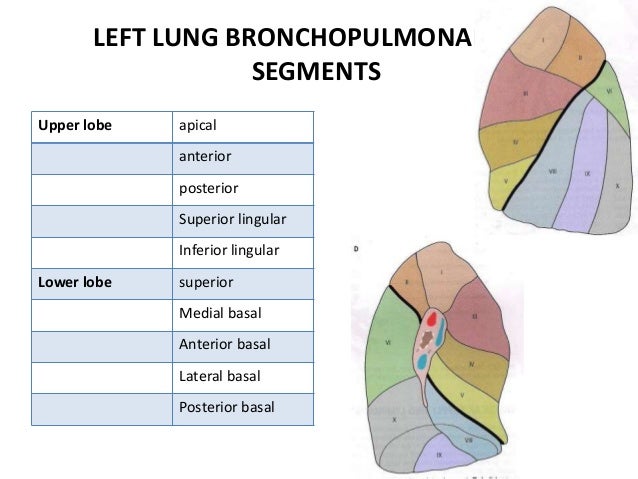
Bronchopulmonary segment:
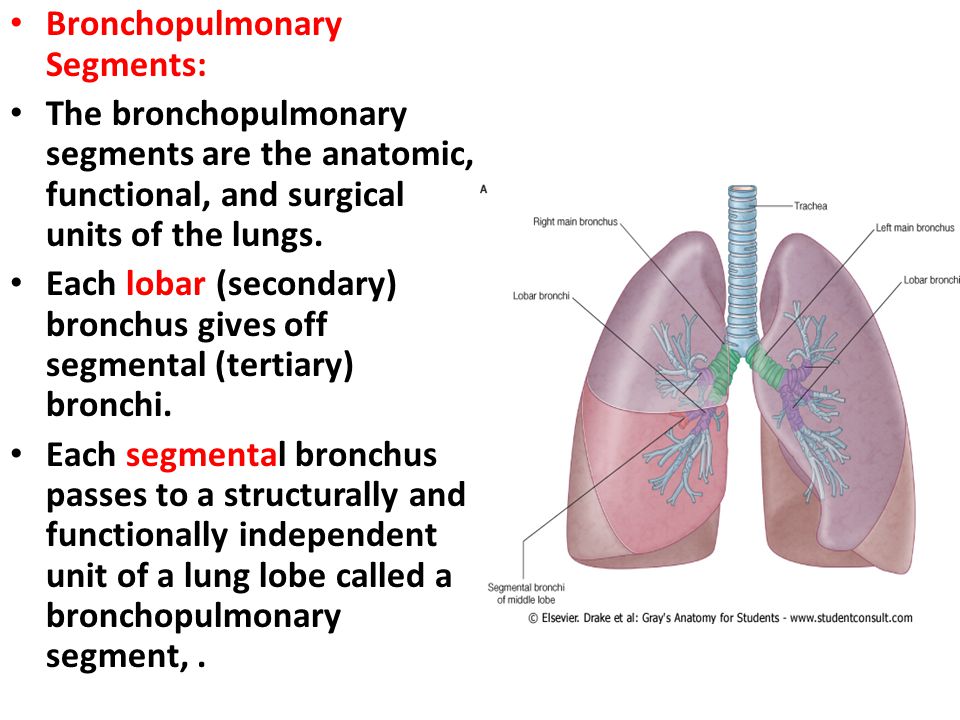
Clinicals: Lung resection – remove specific tumor on segment
Apex of lung – relations:
- Anterior – subclavian artery, scalenus anterior, clavicle
- Posterior – posterior intercostal arteries and veins
- Lateral – 1st rib
- Medial – phrenic nerve, vagus nerve, trachea, esophagus
- Superior – brachial plexus
Right and left lung differences:
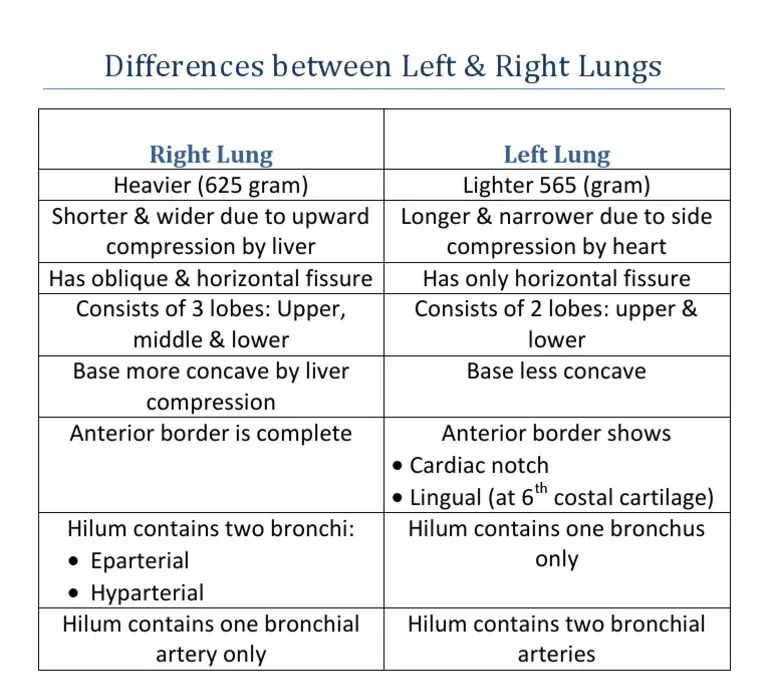
Right – 10 segments, Left – 8 segments
Right and left bronchi:
- Right: Shorter, vertical, 3 divisions, enters lung at T5 level
- Left: Longer, horizontal, 2 divisions, enters lung at T6 level
Right and left hilum:

Right and left lung impressions:

Clinicals:
- Pulmonary embolism – dyspnea, chest pain, cough blood
- Clavicle fractures – damage apex of lungs
- Asthma
- Chronic bronchitis
- Cancer – smoking
- Cystic fibrosis
- Bronchoscopy
- Aspiration of foreign object usually in right principal bronchus as it shorter, wider and more vertical than left
Pericardium
Attachments:
- Anterior – sternopericardial ligament, sternum
- Posterior – posterior mediastinum
- Superior – tunica adventia of great vessels
- Inferior – pericardiophrenic ligament
- Laterally – pulmonary vein adventia
Relations:
- Anterior – sternum, 2-6 costal cartilage
- Posterior – posterior mediastinum
- Superior – thymus, great vessels
- Inferior – pericardiophrenic ligament
- Laterally -phrenic nerve, lungs and pleura pericardiophrenic vessels
Layers:
- Fibrous – prevents over distension of heart
- Parietal – lines pericardium
- Visceral – called epicardium
Sinuses between parietal and visceral layer:

Blood supply:
- Internal thoracic artery – pericardiophrenic and musculophrenic arteries
- Thoracic aorta – bronchial, esophageal, superior phrenic
- Coronary arteries (visceral layer)
Venous:
- Pericardiophrenic – drains into internal thoracic artery
- Azygos venous system
Nerves:
- Fibrous and parietal layer – phrenic nerve, intercostal nerve
- Visceral layer – vagus and sympathetic trunk
Lymphatics: Parasternal, tracheobronchial
Functions of pericardium:
- Fix heart with sternopericardial ligament and pericardiophrenic ligament
- Prevent overfilling of heart
- Lubrication
- Protect from lung infection
Layers of heart wall:
- Fibrous
- Parietal
- Serous fluid
- Visceral/epicardium
- Subepicardial layer
- Myocardium – involuntary striated muscle (Clinicals: myocarditis, infarction)
- Subendocardial layer – Purkinje fibers and vessels
- Endocardium – lines heart cavities and valves (Clinicals: endocarditis)
Clinicals:
- Pericarditis
- Cardiac tamponade – compressed heart and veins
- Pericardial effusion – abnormal accumulation of fluid in the pericardial cavity
- Pericardiocentesis – aspiration of fluid from 5th and 6th intercostal space
Heart
Divided into 1/3 right and 2/3 left by posterior interventricular sulcus, which contains posterior interventricular artery
Borders and surfaces of the heart:
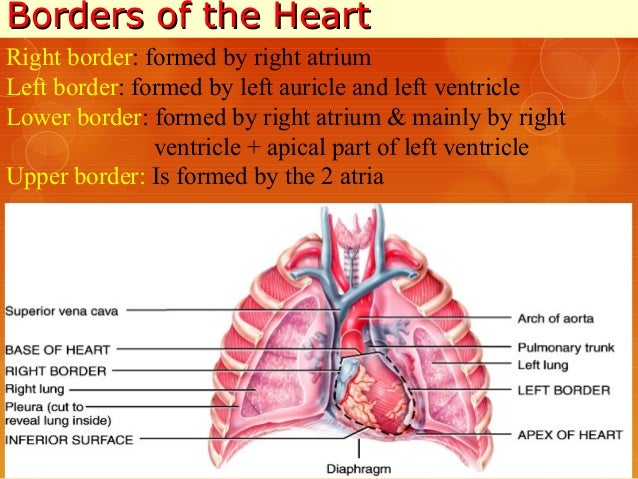

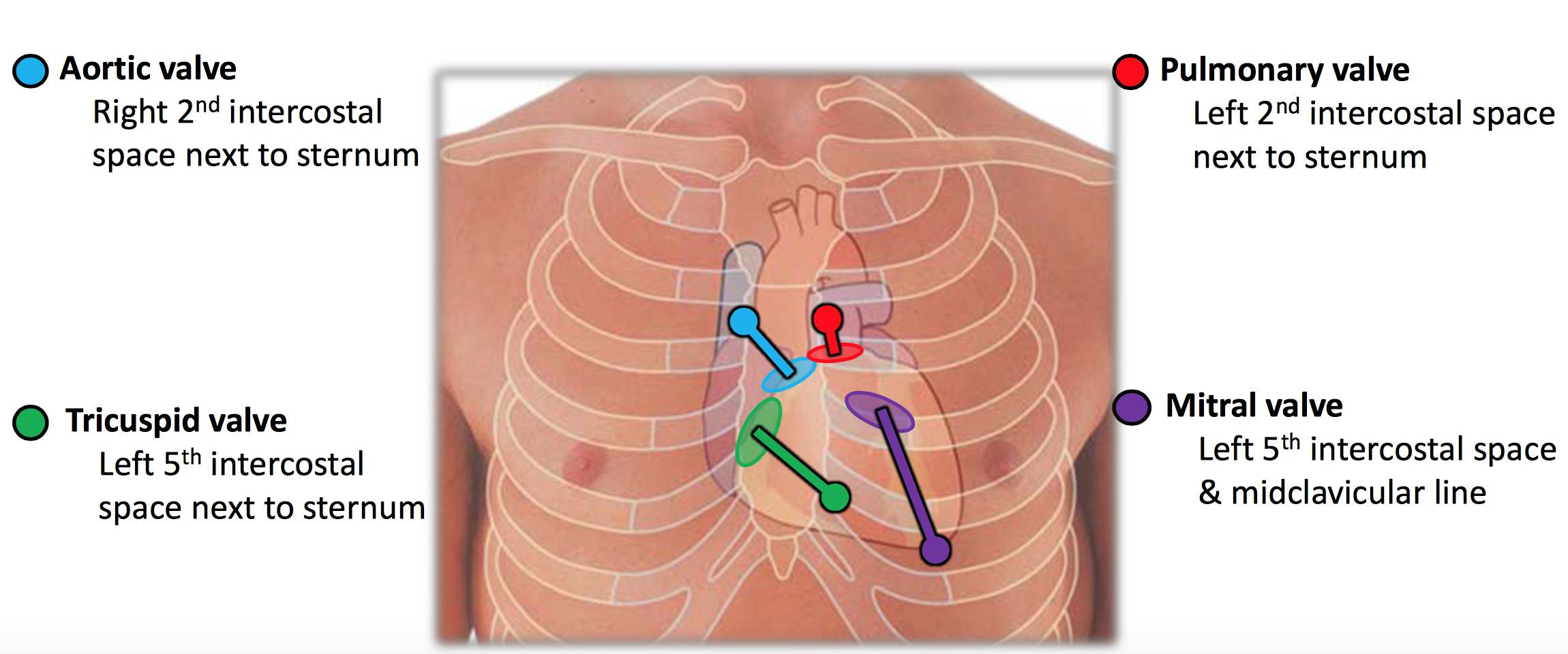
Surface anatomy of the heart:
Blood supply:

Aortic sinus gives off right coronary artery and left coronary artery
Right coronary artery branches:
- Sino arterial nodal
- Right marginal
- AV nodal
- Posterior interventricular
Left coronary artery branches:
- Anterior interventricular
- Circumflex
- Left marginal (from circumflex)
As blood recoils during ventricular diastole, enters coronary arteries to supply heart
NB: Coronary dominance – The coronary artery that supplies SAN, can be right or left or both
Extracardiac anastomosis: Internal thoracic artery branches, bronchial, esophageal, superior and inferior phrenic arteries
Venous:
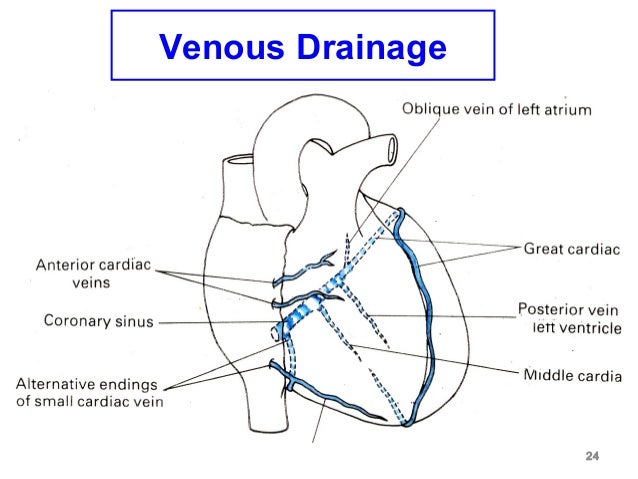
Coronary sinus:
- Runs in posterior coronary groove
- Opens in right atrium between AV orifice and IVC orifice
- Tributaries:
- Great cardiac vein
- Small cardiac vein
- middle cardiac vein
- Left marginal vein
- Left posterior ventricular
- Oblique vein of left atrium
Anterior cardiac veins open directly in right atrium
Lymphatics: Tunica media ⇒ Efferent vessels ⇒ tracheobronchial nodes
Nerves: Sympathetic increases heart rate, parasympathetic decreases
Sympathetic: Right and left cardiac branches of sympathetic ganglia
- Cervical: Superior, middle and inferior ganglia
- Thorax: Ganglia 2,3,4
Parasympathetic:
- Vagus: Right and left upper cervical cardiac branches, right and left lower cervical cardiac branches
- Left recurrent laryngeal – 1 branch
1. Superficial cardiac plexus – Below arch of aorta
- Left superior cervical sympathetic nerve
- Left lower cervical cardiac nerve (parasympathetic)
2. Deep cardiac plexus – infront of tracheal bifurcation
- All the remaining nerves mentioned above

Relations: Same as pericardium
Interior of heart:

(I) Right atrium:
- Crista terminalis (contains SAN)/ Sulcus terminalis – divides atrium into smooth and rough part
- Sinus venarum – smooth – posterior part
- Atrium proper – rough – anterior part
- Pectinate muscles
- SVC, IVC, coronary and AV orifice
(II) Interarterial septum: Fossa ovalis and limbus
Clinicals: Patent foramen ovale
(III) Left atrium:
- Smooth posterior part – absorbed pulmonary veins
- Rough anterior part – Pectinate muscles
(IV) Right ventricle: Divided into 2 by supraventricular crest
- Outflow part – Infundibulum, smooth walls
- Inflow part – Trabeculae carneae which consists of:
- Ridges
- Bridges (eg. moderator band)
- Three Papillary muscles – attached to valves by chorda tendinea – prevents valve prolapse into atria during ventricular systole
(V) Interventricular septum: Superiorly membranous, inferiorly muscular
(VI) Left ventricle:
- Outflow part – Aortic vestibule, smooth walls
- Inflow part – Trabeculae carneae, 2 papillary muscles
Conducting system of the heart:

Triangle of koch: In right atrium, anatomical landmark of AV node
Boundaries: Tendon of Todaro, tricuspid valve and coronary sinus opening

Clinicals:
- Myocardial ischaemia
- Angina pectoris
- Coronary bypass graft – radial artery and long saphenous vein
- Angiogram
- Cardiac referred pain – pain felt in the neck, shoulders, and back
- Heart block 1st, 2nd and 3rd degree
Superior thoracic inlet
Boundaries:
- Anterior – Manubrium
- Posterior – T1 body
- Lateral – 1st rib and costal cartilage
Contents:
- Trachea, esophagus, thoracic duct
- Common carotid artery, subclavian artery and vein, IJV
- Vagus, phrenic, recurrent laryngeal nerves and sympathetic chain
- Apex of lung and pleura
Clinicals: Thoracic inlet syndrome – compression of structures, tumors, enlarged lymph nodes – leads to dysphagia, dyspnea
Inferior thoracic inlet
Boundaries:
- Anterior – 7-10 costal cartilage, xiphisternal joint
- Posterior – T12 body
- Lateral – 11th and 12th ribs
Contents:
- Abdominal aorta
- Azygos vein
- IVC
- Esophagus
- Vagus nerve
- Thoracic duct
Ribcage
(I) Costotransverse and costovertebral joints:

Costotransverse joint – Tubercle of rib articulates with transverse process of corresponding vertebrae
Costovertebral joint – Head of rib articulates with superior costal facet of corresponding vertebrae and inferior costal facet of the vertebra above, as well as the adjacent IVD
(II) Types of ribs:
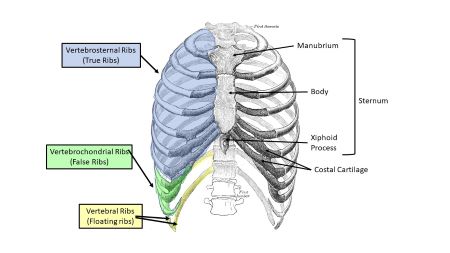
(III) Typical rib:
- Anterior – Costal cartilage (hyaline)
- Posterior – Tubercle and head (2 articular facets)
- Superior – Thick and rounded
- Inferior – Sharp, costal groove

(IV) Atypical ribs:


(V) 1st rib relations:
- Superior – clavicle, subclavian vessels
- Inferior – intercostal vessels
- Medial – sympathetic trunk
(VI) Muscles:
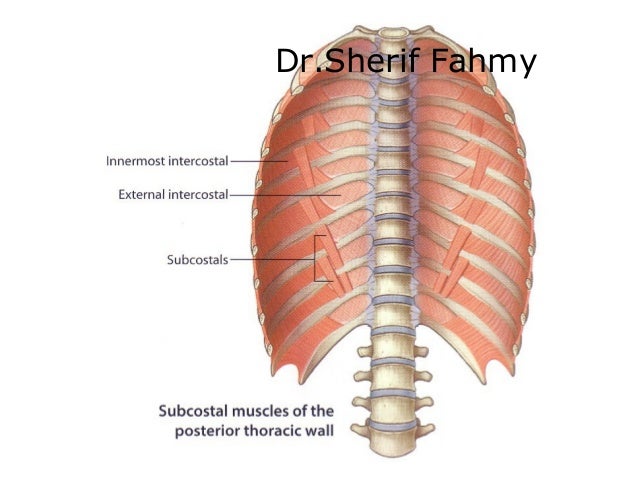
1. Intercostal muscles:

- 11 pairs
- Nerve supply – intercostal nerves (T1-T11)
- Intercostal vein, artery and nerve between internal and innermost intercostal muscles
- External – in inspiration elevate ribcage
- Internal – forced expiration
- Innermost – inspiration
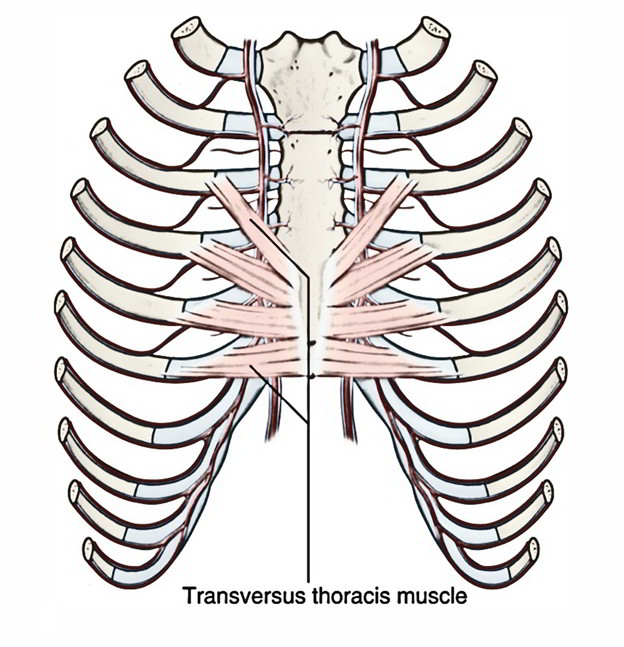
2. Transverse thoracic muscles:
- From posterior inferior sternum to posterior surface of costal cartilage 2-6
- Depress ribs
3. Subcostal muscles:
- From posterior lateral rib to a 2nd or 3rd rib below
- Depress ribs
(VII) Muscles of respiration:

(VIII) Thoracic wall/ Ribcage:
1. Blood supply:
- Thoracic aorta – Posterior intercostals, subcostal artery
- Internal thoracic – Anterior intercostals
- Axillary – Superior and lateral thoracic arteries
2. Venous: Azygos system
3. Nerves:
- Supraclavicular nerve – above 2nd rib
- Anterior rami (T1-T11) intercostal nerves
4. Lymphatics: Intercostal, phrenic nodes
Clinicals:
- Age changes – costal cartilage ossify, xiphoid process ossify
- Paralysis of diaphragm, phrenic nerve damaged – paradoxical movement
- Extra ribs – transverse process of cervical or lumbar vertebrae
- Decreased ribs – failure of 12th rib to form
- Rib fracture – at angle or costal cartilage, most common in ribs 3-10 since they are immobile. 1st and 2nd are protected by clavicle, 11th and 12th are mobile.
- Flail chest – anterolateral chest wall movable due to multiple rib fractures. Moves paradoxically (moves outwards during expiration)
- Funnel chest
- Pigeon chest
- Sternal puncture – to get bone marrow from manubrium, pierces skin, fascia and periosteum. May injure aorta, heart, or pericardium
- Median sternotomy – vertical incision along sternum for heart and lung surgeries
Mediastinum
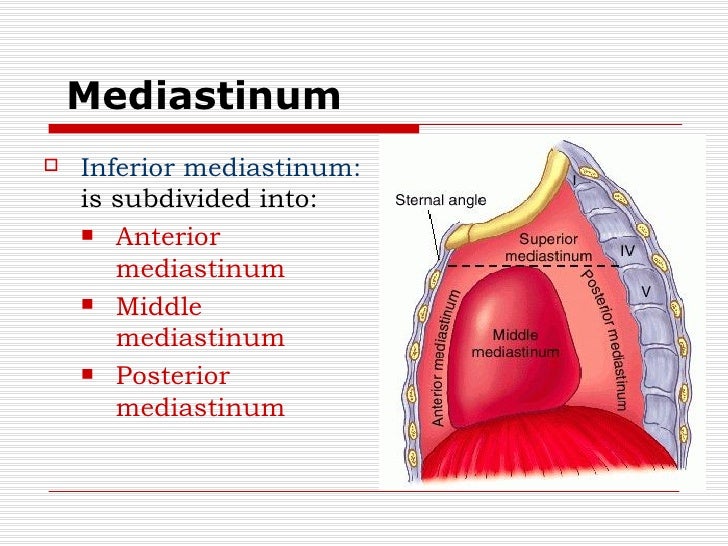
(I) Superior mediastinum:
Relations:
- Superior – Thoracic inlet
- Inferior – Inferior mediastinum
- Anterior – Manubrium
- Posterior – T1-T4
- Lateral – Lungs pleura
Contents:
- Nerves: phrenic, vagus, recurrent laryngeal
- Vessels: SVC, thoracic duct, aorta, internal thoracic artery and vein
- Trachea, esophagus
- Thymus gland
(II) Anterior mediastinum:
Relations:
- Superior – Superior mediastinum
- Inferior – Diaphragm
- Anterior – Sternum
- Posterior – Pericardium
- Lateral – lungs pleura
Contents: Sternopericardial ligament, internal thoracic artery and branches, thymus gland
(III) Middle mediastinum:
Relations:
- Superior – Superior mediastinum
- Inferior – Diaphragm
- Anterior – Pericardium
- Posterior – Pericardium
- Lateral – lungs pleura
Contents: Heart, tracheal bifurcation, phrenic nerve, SVC, pulmonary artery, pulmonary vein, aorta
(IV) Posterior mediastinum:
Relations:
- Superior – Superior mediastinum
- Inferior – Diaphragm
- Anterior – Pericardium
- Posterior – T5-T12
- Lateral – lungs pleura
Contents: Thoracic aorta, thoracic duct, azygos system, esophagus
Vessels and nerves
(I) Internal thoracic artery:
- Originates from 1st part subclavian artery
- Anterior to lung apex
- Enters thorax, posterior to clavicle
- Runs downwards and lateral to sternum
- At 6th intercostal space divides into: superior epigastric (rectus muscle) and musculophrenic (diaphragm)
- Branches: Anterior intercostal arteries, perforators of breast, pericardiophrenic and mediastinal
(II) Aortic arch: (connected to pulmonary trunk by ligament arteriosum)
Location: Sternal angle to lower border T4
Relations:
- Superior – Brachiocepahlic trunk, left common carotid, left subclavian artery
- Inferior – Pulmonary trunk
- Left/anterior – Pleura, phrenic nerve and vagus nerve
- Right posterior – trachea, esophagus
Branches: Brachiocepahlic trunk, left common carotid, left subclavian artery, right and left coronary arteries
(III) Thoracic aorta:
Location: Posterior mediastinum (T4-T12)
Relations:
- Anterior – Pericardium
- Posterior – Vertebral column
- Right – Thoracic duct, azygos vein
- Left – Left lung and pleura
Branches: Posterior intercostals, bronchial, esophageal, pericardial, mediastinal, superior phrenic, subcostal
(IV) Brachiocephalic trunk:
Location: Posterior to manubrium
Relations:
- Anterior – Manubrium
- Posterior – Trachea
- Right – SVC
- Left – Left common carotid
Branches: Right common carotid and right subclavian
(V) SVC:
Extent: 1st-3rd costal cartilage
Location: Anterior and right of superior mediastinum
Relations:
- Anterior – Ascending aorta, right lung
- Posterior – Trachea
- Lateral – Right lung and pleura
Tributaries: Right and left brachiocephalic veins, azygos vein, right and left supreme intercostal veins
(VI) Azygos venous system:
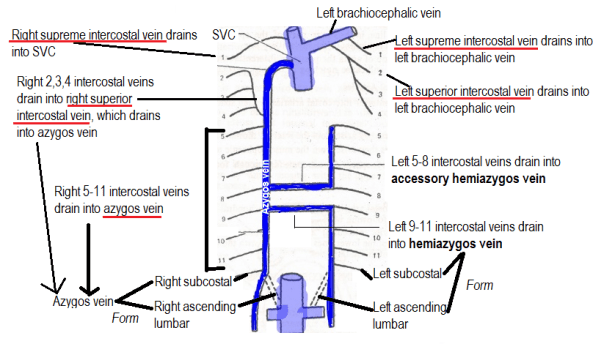
- Azygos vein formed from right subcostal vein and right ascending lumbar vein
- Hemiazygos and accessory hemiazygos drain into azygos vein
- Azygos vein enters thorax via aortic hiatus
- Ascends right of T12 – T4
- Drains into SVC
(VII) Thoracic duct: Main lymphatic trunk
- Continues as cisterna chyli in abdomen
- Enters thorax via aortic hiatus
- In posterior mediastinum, right to thoracic aorta snd posterior to esophagus
- Crossed from right to left at T4
- In superior mediastinum
- Joins junction of left IJV and left subclavian to form left brachiocephalic vein
Territory of drainage: all except superior right quadrant
Clinicals: Laceration – thin wall tears, chyle accumulates in posterior mediastinum
(VIII) Phrenic nerve:
- Origin: Anterior rami of C3,C4,C5
- Begins at lateral border of anterior scalene muscle
- Descends anterior to anterior scalene, deep to prevertebral layer
Right phrenic nerve:
- Passes anterior to 2nd part of subclavian artery
- Enters thorax via superior mediastinum
- Right side of brachiocephalic vein, SVC and pericardium
- Descends anterior to lung root
- Pierce diaphragm near caval opening
Left phrenic nerve:
- Passes anterior to 1st part of subclavian artery
- Enters thorax via superior mediastinum
- Crosses aortic arch and vagus nerve
- Descends anterior to lung root
- Pierce diaphragm
Phrenic nerve distribution:
- Motor and sensory – Diaphragm
- Sensory:
- Parietal pleura
- Parietal pericardium
- IVC
- Suprarenal glands
- Biliary apparatus
Clinicals: Referred pain
(IX) Thoracic sympathetic chain:
- Runs over neck of ribs and transverse process of vertebrae
- Pierce diaphragm to supply abdomen
Trachea, esophagus and thymus gland
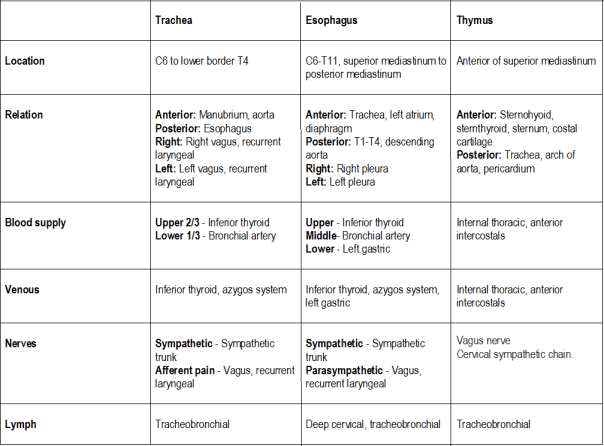
Esophagus:
Constrictors: Cricopharyngeal sphincter, arch of aorta, left main bronchus, diaphragmatic constriction
Clinicals of esophagus: Cancer, compression due to right atrium hypertrophy – dysphagia
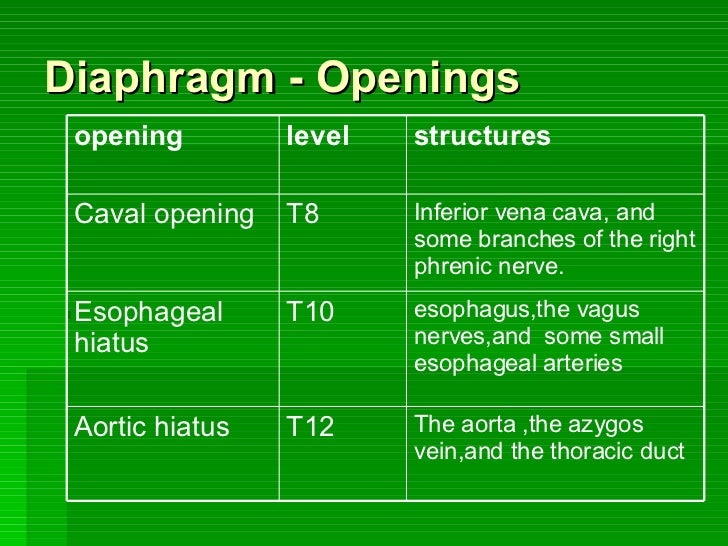
Diaphragm
Attachments:
- L1 and L2
- 7-12 rib’s costal cartilage
- Xiphoid process of sternum
- Right (L1-L3) and left (L1-L2) crus – combine to form central tendon
Openings:

Blood supply:
- Internal thoracic – Pericardiophrenic, musculophrenic
- Thoracic aorta – Superior phrenic
- Abdominal aorta – Inferior phrenic
- Lower intercostal arteries
Nerves: Phrenic (motor), intercostal nerves and subcostal nerve (sensory)
Lymphatics: Parasternal, anterior and posterior diaphragmatic
Action:
- Contract, flatten
- Relax, dome shaped
Functions of diaphragm:
- Muscle of inspiration – increase verticle diameter
- Muscle of abdominal straining – helps anterior abdominal muscles to contract, therefore raise intraabdominal pressure for micturition, defecation or parturition
- Weight lifting muscle
- Thoracoabdominal pump – as diaphragm increases intraabdominal pressure and decreases intrathoracic pressure, it compresses blood in IVC and forces it upwards. Thoracic duct also aided.
Relations:
- Superior – Pericardium, lungs
- Inferior – Liver, adrenals, kidney, stomach, spleen
- Posterior – Aorta, azygos vein, esophagus
Clinicals:
- Paralysis (suffocation)
- Hiccups -involuntary contractions of diaphragm, irritation
- Referred pain – shoulder region
- Hiatal hernia – stomach enters thorax via th esophageal hiatus
- Median arcuate ligament syndrome – abdominal pain due to compression of celiac artery
These are summarized notes from various sources, mainly TeachMeAnatomy and Wikipedia
Anatomy of Head and Neck
Arteries
1. Blood supply of face:

- External carotid artery branches ^^
- Ophthalmic artery branches: supratrochlear, supraorbital
2. Ophthalmic artery:
- 1st branch of internal carotid artery
- Through optic canal
- Runs in medial wall of orbit
- Branches:
- Lacrimal
- Central retinal
- Supratrochlear
- Supraorbital
3. Maxillary artery:
- Branch of external carotid artery, arises behind neck of mandible
1st part (mandibular):
- Passes between mandible ramus and sphenomandibular ligament
- Branches:
- Deep auricular
- Anterior tympanic
- Inferior alveolar
- Middle meningeal
- Accessory meningeal
2nd part (pterygoid):
- Passes between 2 heads of lateral pterygoid muscle and enters pterygoid fossa
- Branches:
- Masseteric
- Deep temporal
- Pterygoid
- Buccal
3rd part (pterygomaxillary):
- Lies in pterygopalatine fossa
- Branches:
- Sphenopalatine artery
- Greater and lesser palatine arteries
- Posterior superior alveolar artery
- Pharyngeal artery
- Infraorbital artery
4. Facial artery:
- Emerges in carotid triangle from external carotid artery (ECA)
- Deep to mandible ramus
- Superficial to masseter and buccinator
- Ascends lateral nose
- Becomes angular artery
- Branches:
- Superior labial
- Inferior labial
- Lateral nasal
- Angular
5. Subclavian artery:
- Right one arises from brachiocephalic artery, left one arises from arch of aorta
- It is divided into 3 parts as it passes posterior to anterior scalene muscle
- Branches:
- 1st part – Vertebral, internal thoracic, thyrocervical
- 2nd part – Superior intercostal, deep cervical
- 3rd part – Dorsal scapular
- Continues as axillary artery at border of 1st rib
6. Common carotid artery:
- Right from brachiocephalic trunk, left from arch of aorta
- Bifurcates into ECA and ICA at superior border of thyroid cartilage
7. External carotid artery:
- Formed from common carotid artery
- At upper border of thyroid cartilage
- Outside carotid sheath
- Posterior to ramus of mandible
- Terminates as superficial temporal and maxillary artery
8. Vertebral artery:
- From subclavian artery 1st part
- Through vertebral triangle
- Ascend in transverse foramina C6-C1
- Enter cranial cavity via foramen magnum
- Joins other side’s vertebral artery to form basilar artery at base of pons
Veins
1. Venous drainage of face

2. Facial vein:
- Tributaries: Supraorbital and supratrochlear drain into angular vein
- Becomes facial vein
- Superficial to masseter, buccinator and mandible
- Joins anterior division of retromandibular vein
- To form common facial vein
- Drains into IJV
3. External jugular vein (EJV):
- Formed from retromandibular vein, posterior division and posterior auricular vein
- Forms at angle of mandible
- Pierce deep fascia
- Drain into subclavian vein
4. Internal jugular vein (IJV):
- Formed from sigmoid sinus and inferior petrosal sinus
- Through jugular foramen
- Runs in carotid sheath
- Unites with subclavian vein to form brachiocephalic vein
- Tributaries: Common facial, lingual, pharyngeal, superior and middle thyroid veins
5. Subclavian vein:
- Continuation of axillary vein from border of 1st rib
- Anterior to scalenus anterior muscle
- Joins IJV and EJV to form brachiocephalic vein
Nerves
1. Nerve supply to face:
- Motor – facial nerve branches
- Sensory – trigeminal nerve and nerves C2, C3, C4
2. Inferior alveolar nerve:
- Branch of V3
- Gives off a branch – mylohyoid nerve (mylohyoid and anterior diagastric muscle)
- Between mandible ramus and medial pterygoid muscle
- Enters mandible foramen, through mandible canal
- Through inferior dental plexus
- Gives off a mental nerve (at mandibular 2nd premolar) which exits via mental foramen (sensory to chin and lower lip)
- Continues as mandibular incisive nerve to innervate mandibular canines and incisors
Clinicals:
- Inferior alveolar nerve block – anesthesia near mandibular foramen
- Injury – 3rd molar removal, dental implants, root canal
3. Lingual nerve:
- Branch of V3
- Chorda tympani nerve (of facial nerve) joins lingual nerve
- Between mandible ramus and medial pterygoid muscle
- Inferior to 3rd molar
- Runs between hyoglossus muscle and deep part of submandibular gland
- Crosses lateral to medial over Wharton’s duct
- Runs along tip of tongue becoming sublingual nerve, lying beneath mucous membrane
Clinical: 3rd molar surgery – injury to nerve
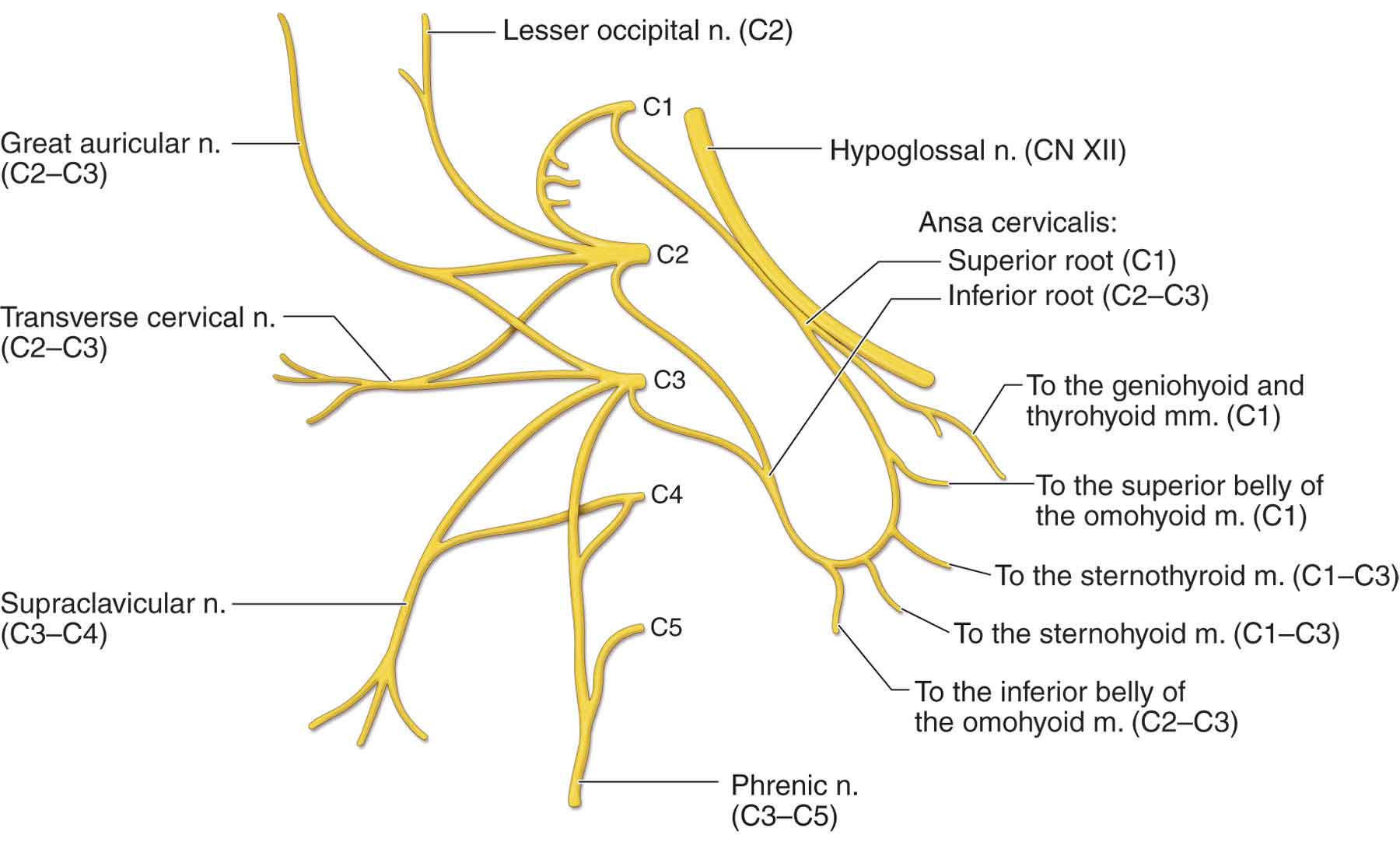
4. Cervical plexus:
Anterior rami C1-C4 – in carotid triangle
5. Gustatory pathway:

Waldeyer’s ring

Palatine tonsils:
- Location: Between palatoglossus and palatopharyngeus folds
- Relations:
- Anterior – palatoglossus fold
- Posterior – palatopharyngeus fold
- Superior – soft palate
- Inferior – tongue
- Lateral – superior constrictor
- Blood supply:
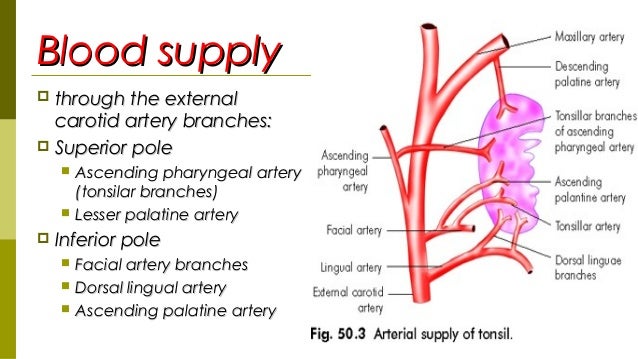
- Nerve: Glossopharyngeus nerve, lesser palatine nerve (V2)
Clinicals: Tonsillitis, tonsilectomy
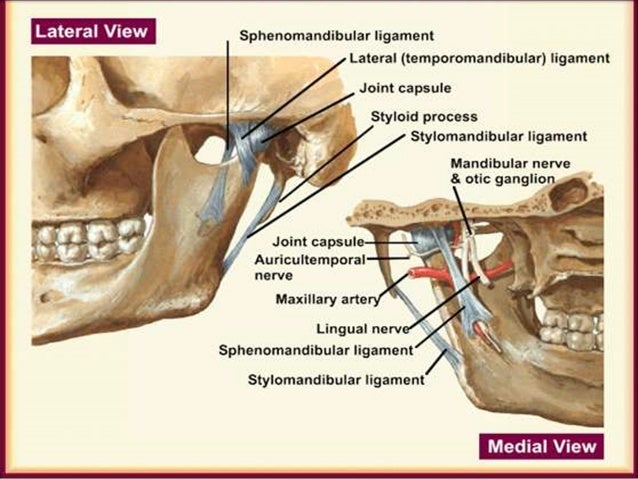
Temporomandibular joint (TMJ)
Lateral pterygoid muscle attatches to TMJ capsule – slide forward movement
Classification: Synovial modified hinge
Lined by: Fibrocartilage
Articular surfaces: Condyle, mandibular fossa and articular tubercle of squamous temporal

Stability factors:
Static:
- Mandibular fossa and posterior glenoid tubercle
- Articular disc – attaches to internal surface of joint capsule, dividing it into superior and inferior cavity
- Condyle head more convex antero-posteriorly than medial to lateral
- Lateral pole more anterior than medial
- Ligaments:
- Lateral ligament – from articulating eminence to posterior condyle, prevents extreme retrusion
- Lateral and medial collateral ligament
- Sphenomandibular ligament – from sphenoid spine to lingula, prevents extreme protrusion
- Stylomandibular ligament – from styloid process to angle of mandible
Dynamic: Muscles of mastication
Blood supply: Superficial temporal and masseteric arteries
Nerve supply: Auriculotemporal and masseteric
Movements: Rotation, Protraction
Relations:
- Anterior – lateral pterygoid muscle
- Posterior – parotid gland
- Lateral – parotid gland
- Medial – spine of sphenoid
- Superior – middle cranial fossa
- Inferior – maxillary artery
Glands
(I) Lacrimal gland:
Blood supply: Lacrimal artery from opthalmic artery
Nerve supply:

(II) Parotid gland:
Relations:
- Superior – zygomatic arch
- Inferior – mandible angle
- Anterior – masseter muscle
- Posterior – sternocleidomastoid muscle (SCM)
- Roof – skin and fascia
- Floor – masseter, SCM, mandible ramus
Stenson’s duct course: Anterior to masseter, pierce buccinator, open in vestibule next to 2nd maxillary molar
Pierced by: Superficial temporal artery, retromandibular vein, facial nerve
Blood supply: Superficial temporal artery
Venous: Retromandibular vein
Nerve supply:

- Parasympathetic: Lesser petrosal nerve
- Sympathetic: Superior cervical ganglion
Lymphatic drainage: Posterior and preauricular lymph nodes
Type of secretion: Serous
Clinicals:
- Parotid gland tumor
- Parotiditis – inflammation
- Mumps
(III) Submandibular gland:
Location: Submandibular triangle
Relations:
- Superior – mylohyoid line
- Inferior – diagastric tendon
- Anterior – mental foramen
- Posterior – mandible angle
- Medial – root of tongue
- Lateral- masseter and mandible
Wharton’s duct course: Through 3 muscles (mylohyoid, hyoglossus, genioglossus) ⇒ crossed by lingual nerve ⇒ opens near frenulum
Nerve supply:
- Parasympathetic: Vasodilation
- Sympathetic: Vasoconstrict, therefore enzyme rich mucous
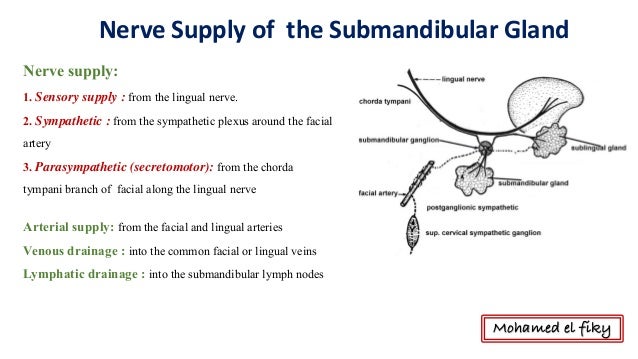
Lymphatic drainage: Submandibular lymph nodes, which drain to jugulodiagastric lymph nodes
Type of secretion: Serous and mucous (seen as demilunes in histology)
Clinicals:
- Submandibular excision – damage lingual and facial nerve
- Calcified stones – due to ascending duct, serous and mucous secretions, and it’s a long duct
(IV) Sublingual gland:
Location: Sublingual fossa above mylohyoid line
Relations:
- Superior – mucous membrane of mouth
- Inferior – mylohyoid muscle
- Posterior – submandibular gland
- Medial – genioglossus muscle
- Lateral- sublingual fossa
Blood supply, venous drainage, nerve supply and lymph nodes – same as submandibular gland
Type of secretion: Mucous – sublingual papilla
Clinicals:
- Ranula – mucous cysts in floor of mouth
(V) Thyroid gland:
Location: Anterior neck, below laryngeal prominence
Extent: C5-T1
Relations:
- Anterior – sternohyoid, sternothyroid
- Posterior – trachea
- Superior – cricothyroid cartilage
- Inferior – 5 tracheal rings
- Medial – esophagus
- Lateral – carotid sheath
Blood supply: Superior, middle, inferior thyroid artery and vein
Nerves:
- Sympathetic: Cervical sympathetic ganglions (superior, middle, inferior)
- Parasympathetic: Vagus nerve
Lymphatics: Pretracheal, paratracheal and prelaryngeal lymph nodes

Clinicals:
- Goiter – enlarged thyroid gland
- Thyroidectomy – surgical removal
- Tracheotomy – forming an opening into trachea due to sudden obstruction of vital airways
- Laryngoscopy
Muscles
(I) Extraocular muscles:

Blood supply: Ophthalmic artery
Nerve supply: Oculomotor, Trochlear (superior oblique), Abducens (lateral rectus)
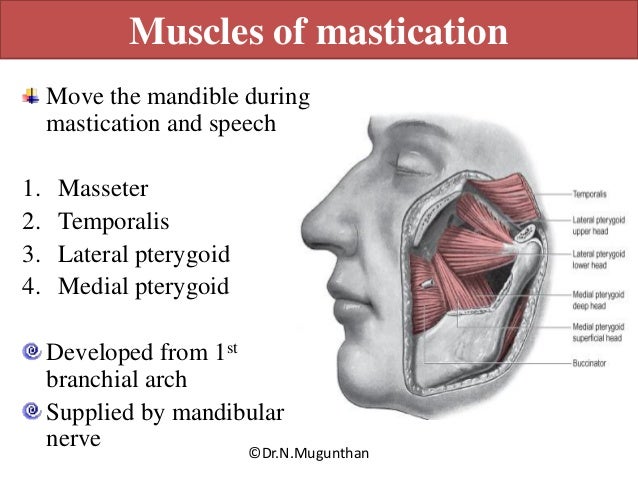
(II) Muscles of mastication:

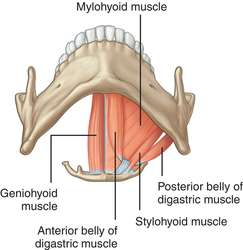
(III) Suprahyoid muscles:

(IV) Infrahyoid muscles:



(V) Sternocleidomastoid (SCM):
- Origin: 2 heads – manubrium, medial 1/3 clavicle
- Insertion: mastoid process
- Innervation: CN 11
- Action: Turn head opposite side, raise thorax
- Relations:
- Anterior – platysma muscle
- Posterior – carotid sheath
- Medial – ansa cervicalis
- Lateral – subclavian artery
(VI) Scalenus anterior:
- Origin: Transverse process C3-C6
- Insertion: 1st rib, scalene tubercle
- Innervation: Anterior rami C4-C6
- Relations:
- Anterior – SCM, subclavian vein
- Posterior – 2nd part subclavian artery, brachial plexus
- Medial – 1st part subclavian artery
- Lateral – 3rd part subclavian artery, brachial roots
Clinicals: Scalenus anterior syndrome – hypertonic muscle, compresses structures
Spaces
(I) Orbit:
Boundaries:

Foramens/fissures and their contents:

Orbit contents: Extraocular muscles and ciliary ganglion
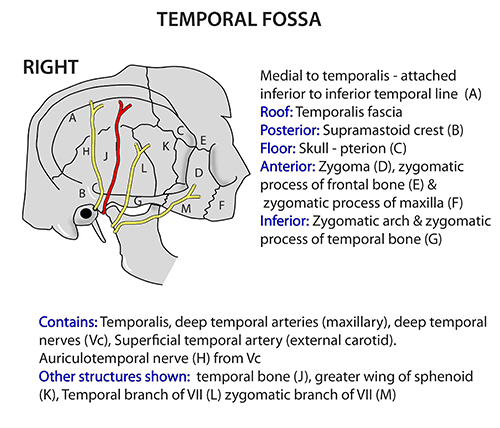
(II) Temporal fossa:
(III) Infratemporal fossa:

Contents: Lateral and medial pterygoid muscles, maxillary artery, mandibular nerve, otic ganglion
(IV) Pterygopalatine fossa:


Clinicals: Ligate sphenopalatine artery to stop nose bleeding
(V) Neck triangles:
(A) Anterior neck triangles
Boundaries:

NB: Submandibular, Carotid and Muscular triangle are paired. Submental triangle is the only unpaired triangle.
Contents:
Submental triangle:
- Submental lymphnodes
Submandibular (diagastric) triangle:
- Hypoglossal nerve
- Nerve to the mylohyoid
- Marginal mandibular branch of the facial nerve (MMB)
- Facial and lingual arteries and veins
- Submandibular gland
- Lower pole of the parotid gland
- Submandibular lymph nodes
Carotid triangle:
- Common carotid artery (and its bifurcation into ECA & ICA)
- Arteries: Superior thyroid, lingual, facial, occipital, and ascending pharyngeal arteries
- Veins: Superior thyroid, lingual, facial, ascending pharyngeal, and occipital veins – Drain into IJV
- Nerves: Hypoglossal nerve, the external and internal branches of the superior laryngeal nerve arising from the vagus nerve
Muscular triangle:
- Muscles: Sternohyoid, sternothyroid, omohyoid, and thyrohyoid muscles
- Superior thyroid artery
- Anterior jugular and inferior thyroid veins
- Ansa cervicalis
- Anterior cervical, infrahyoid, prelaryngeal, thyroid, pretracheal, paratracheal lymph nodes
- Medial part: Esophagus, trachea, thyroid gland, and the lower part of the larynx.
(B) Posterior neck triangles
Boundaries:

- Roof: Investing fascia
- Floor: Anterior, middle and posterior scalene muscles
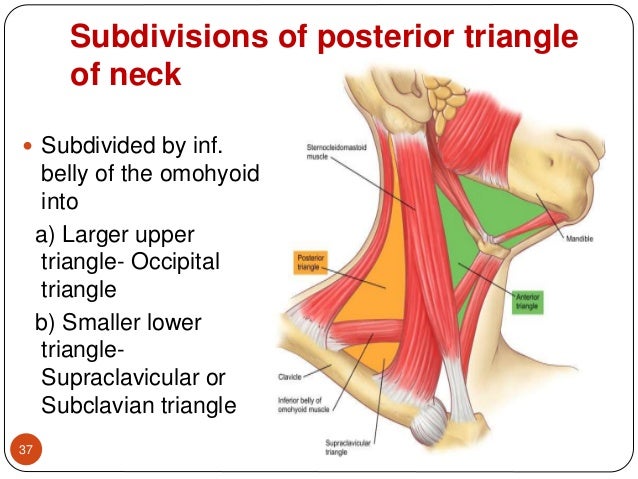
Contents:
- Occipital: Brachial roots, cervical plexus, occipital artery
- Subclavian: Subclavian artery and vein, EJV, brachial plexus trunks
(VI) Interscalene triangle:
- Boundaries: Anterior scalene, middle scalene, 1st rib
- Contents: Subclavian artery, brachial plexus roots
(VII) Suboccipital triangle:
Boundaries:

Contents: Vertebral artery, suboccipital venous plexus
Clinicals: Angiography of circle of Willi’s
Nasal cavity:

Extent: Vestibule to nasopharynx
3 parts: Vestibule, olfactory region, respiratory region
Functions:
- Humidify air – rich vascular supply
- Conchae slow down air
- Prevent pathogens
- Smell
- Drain paranasal sinus
Boundaries:
- Superior – ethmoid and sphenoid bone
- Inferior – palatine bone
- Medial – septa
- Lateral – conchae
Below superior, middle and inferior conchae are meati (openings)

Openings in the meati:
- Above superior conchae/ sphenoethmoidal recess – Sphenoidal sinus
- Superior meatus – Posterior ethmoidal sinus
- Middle meatus – Frontal, maxillary and anterior ethmoidal sinus
- Inferior meatus – Auditory tube, nasolacrimal duct
Other openings:
- Cribriform plate – olfactory nerves
- Sphenopalatine foramen (connects pterygopalatine fossa) – sphenopalatine artery, nasopalatine nerve
- Incisive canal (connects oral cavity) – nasopalatine nerve to oral cavity
Blood supply:
- Internal carotid artery: Anterior and posterior ethmoidal via cribriform plate
- External carotid artery:
- Maxillary artery – Sphenopalatine, greater palatine
- Facial artery – Superior labial, lateral nasal
Venous: Ophthalmic vein, angular vein, sphenopalatine vein
Nerves:
- Smell – olfactory
- General sensory – nasopalatine, nasociliary (V2)
Clinicals: Spread of respiratory infection to ear
Paranasal sinuses:

- Air filled extensions of nasal cavity
- Reduce weight of skull
- Humidify air
- Are paired
- Are mucous lined

Clinicals:
- Sinusitis
- Inflammation of maxillary sinus – tooth ache
- Rhinitis – inflamed nasal mucosa
- Epistaxis – nose bleed (trauma or hypertension)
Tongue:
4 types of papillae:

- Filiform – all over the tongue, only type that contain no taste buds
- Fungiform – mushroom shaped, concentrated on tip of tongue
- Foliate – found on postero-lateral surface of tongue
- Circumvallate – 12 to 14, anterior to sulcus terminalis, Von Ebner’s glands open in it
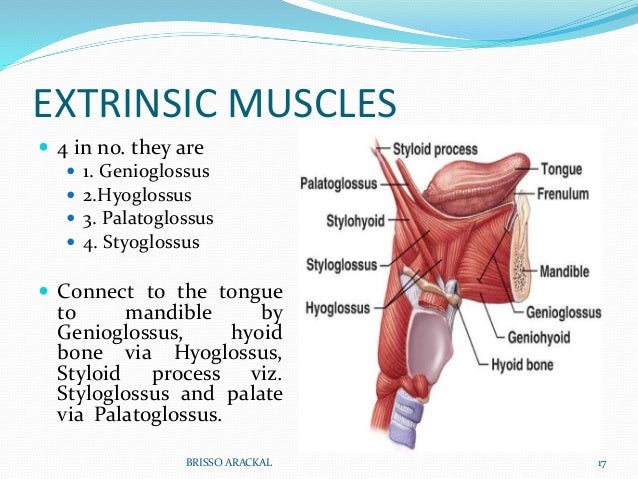
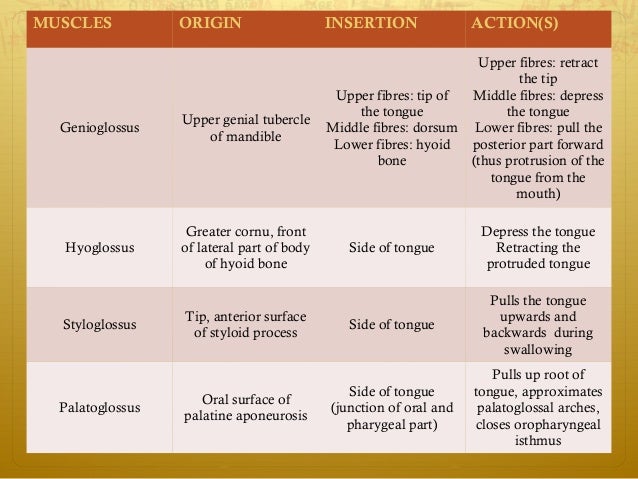
Extrinsic muscles:
Intrinsic muscles:


Blood supply: Lingual artery and vein
Nerve supply:
- Taste: Anterior 2/3 chorda tympani nerve, Posterior 1/3 glossopharyneal nerve
- General sensation: Anterior 2/3 Lingual nerve (V3), Posterior 1/3 glossopharyneal nerve
- Motor: Hypoglossus nerve, except palatoglossus muscle which is supplied by vagus nerve
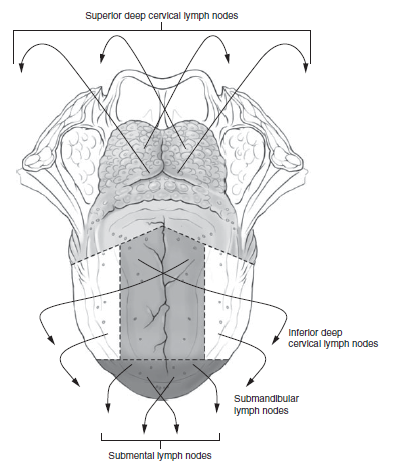
Lymphatic drainage: Superior deep cervical, inferior deep cervical, submandibular, submental lymph nodes
Clinicals:
- Tongue tie
- Cancer
- Halitosis – bad breath
- Oral thrush
Hard palate and soft palate
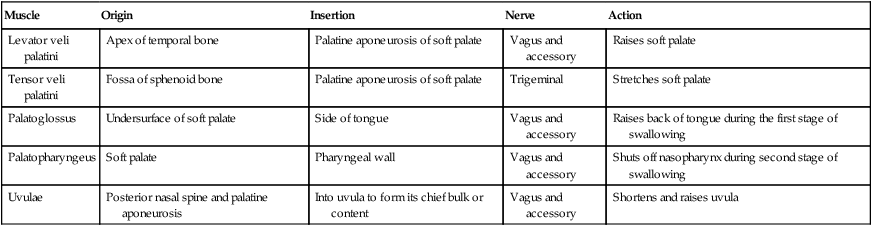
Soft palate muscles:
Blood supply:
Hard palate: Greater palatine artery (from descending palatine)
Soft palate:
- Greater/ lesser palatine (from maxillary artery)
- Ascending palatine (from facial artery)
- Ascending pharyngeal (from ECA)
Veins: Drain into pterygoid venous plexus
Nerves:
Hard palate:
- Greater palatine – mucosa of posterior hard palate (from pterygopalatine ganglion, descends through greater palatine foramen with greater palatine artery)
- Nasopalatine – anterior mucosa (through incisive foramen)
Soft palate:
- Pharyngeal plexus via vagus nerve
- Except tensor veli palatini – medial pterygoid nerve (V3)
- Sensory – Lesser palatine nerve
Lymphatic drainage:
Hard palate: Submandibular, superior deep cervical nodes
Soft palate: Retropharyngeal, superior deep cervical nodes
Clinicals:
- Cleft palate
- Palatal abscesses
- Cleft uvula
- Pimples on hard palate
Pharynx
Extent: Base of skull to C6
Layers:
- Buccopharyngeal fascia
- Muscular layer – outer circular, inner longitudinal
- Pharyngobasilar fascia
- Submucosa
- Mucosa
- Surface epithelium
Muscles:


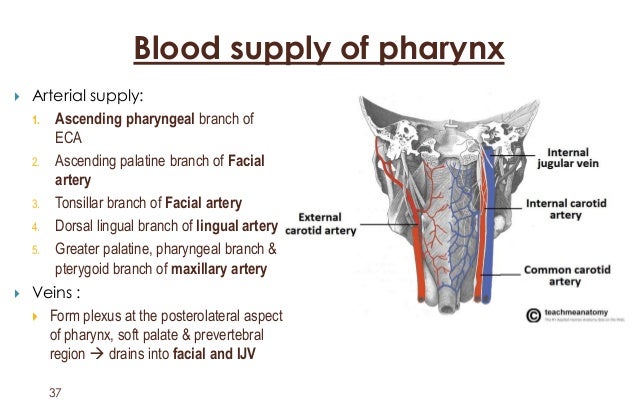
Blood supply:
Nerve:
Motor:
- Glosopharyngeal – Stylopharyngeus muscle
- Vagus – Rest of pharynx muscles
Sensory:
- Nasopharynx – Maxillary (V2)
- Oropharynx – Glossopharyngeal
- Laryngopharynx – Vagus
Lymphatics: Upper and lower deep cervical lymph nodes, retropharyngeal nodes
Clinicals:
- Tonsillitis
- Pharyngeal diverticulum – cricopharyngeus does not relax, food accumulates, dysphagia
- Tumors – dysphagia, dysphonia
Nasopharynx, oropharynx, laryngopharynx


Larynx

- Phonation
- Cough reflex
- Protect respiratory tract
Extent: C3-C6
Relations:
- Anterior – infrahyoid muscles
- Posterior – trachea
- Lateral – thyroid lobes
Made of 6 cartilages: (all are hyaline cartilage except epiglottis)
Single:
- Thyroid – has laryngeal prominence
- Cricoid – encircles completely at C6
- Epiglottis – elastic cartilage
Paired:
- Arytenoid
- Corniculate
- Cuneiform
Ligaments/membranes:
Extrinsic:
- Thyrohyoid membrane – pierced by internal laryngeal nerve and superior laryngeal vessels
- Median cricothyroid ligament
- Cricotracheal ligament
Intrinsic:
- Cricothyroid/vocal ligament
- Quadrangular ligament
NB: Vocal opening – Rima glottidis
Blood supply:
- Superior laryngeal artery(from superior thyroid artery) – runs with internal laryngeal nerve
- Inferior laryngeal artery(from inferior thyroid artery) – runs with recurrent laryngeal nerve
Venous:
- Superior laryngeal – drains in superior thyroid
- Inferior laryngeal – drains in inferior thyroid
Nerves:
Sensory:
- Infraglottis – Recurrent laryngeal
- Supraglottis – Internal laryngeal
Motor:
- Cricothyroid muscle – External laryngeal
- All other muscles – Recurrent laryngeal
Sympathetic: Middle and inferior cervical sympathetic ganglia
Clinicals:
- Cricothyroidotomy- Make temporary airway
- Laryngitis
- Laryngectomy
- Laryngoscopy
- In puberty, boy’s cartilage enlarge, vocal folds become thicker
- Old age – ligament and cartilage ossify
Others
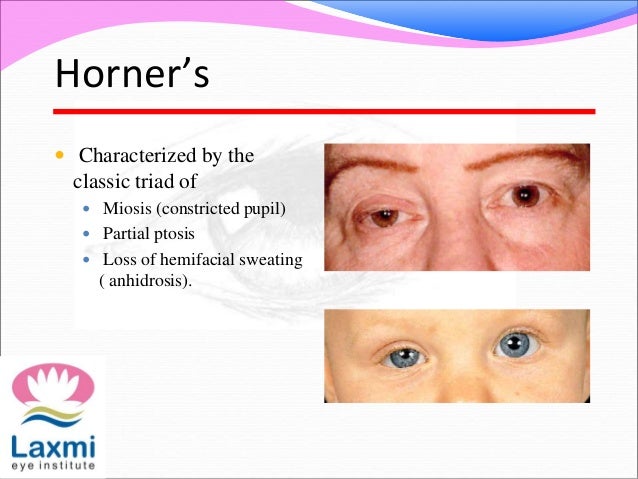
1. Horner’s syndrome:
2. Deep fascia of neck:

3. Structures in midline of neck:
Hyoid bone ⇒ Thyrohyoid membrane ⇒ Thyroid cartilage ⇒ Cricothyroid membrane ⇒ Cricoid cartilage ⇒ Cricotracheal ligament ⇒ Tracheal rings

NB: Internal laryngeal artery and superior laryngeal vessels pierces thyrohyoid membrane
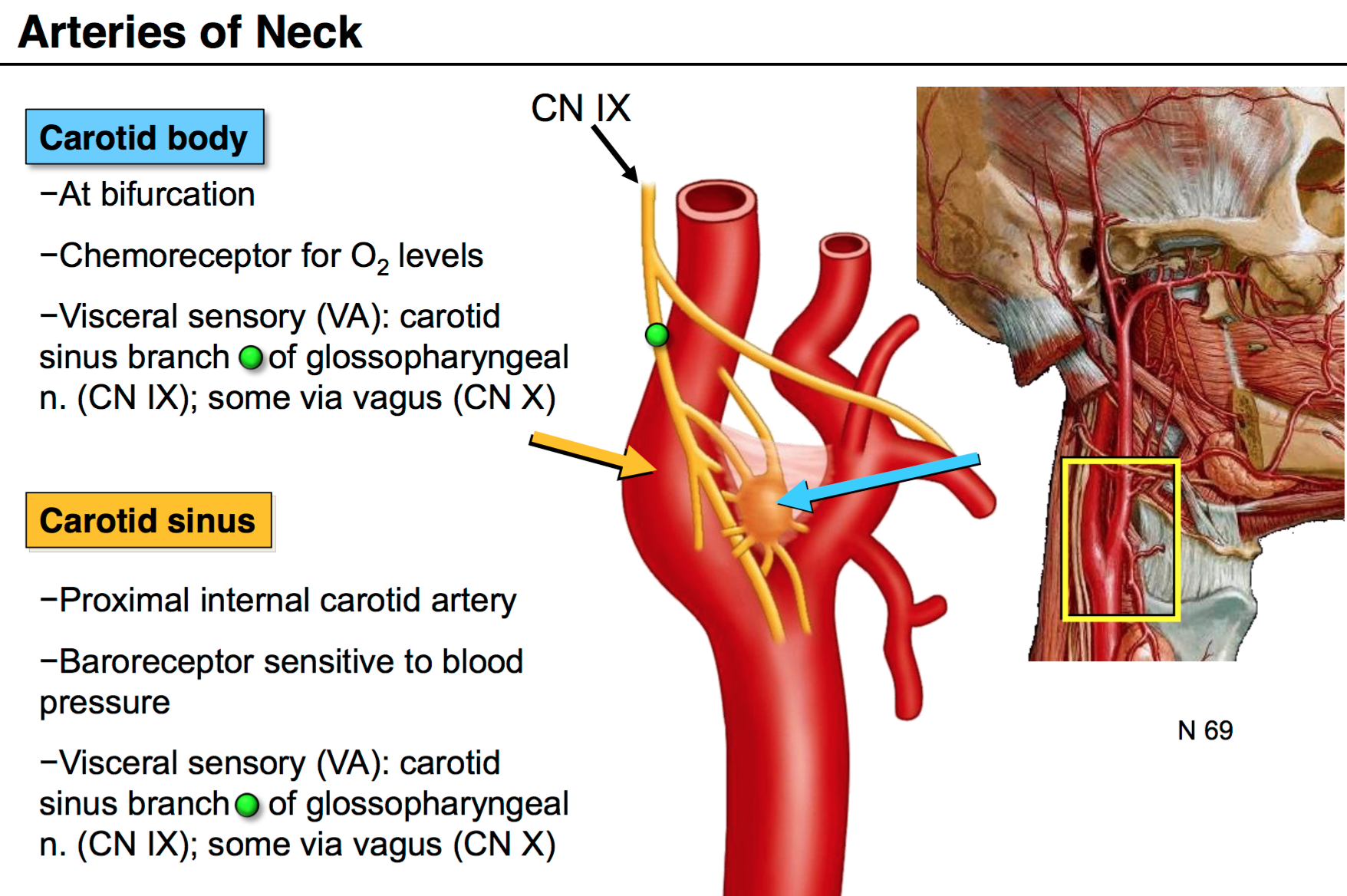
4. Carotid body and carotid sinus:
5. Parts of mandible:

6. External and internal auditory meatus:

EAM to tympanic cavity:
- Blood supply: Posterior auricular, superficial temporal
- Nerve: Great auricular, auriculotemporal
IAM:
- Blood supply: ascending pharyngeal
- Nerve: Glossopharyngeal
Clinicals:
- Otitis – ear inflammation
- Mastoiditis – middle ear infection
7. Fascial space infection:
These are summarized notes from various sources, mainly TeachMeAnatomy and Wikipedia
Tractology Anatomy



Ascending pathways
- 1st, 2nd and 3rd order
- Lesions before decussation – ipsilateral paralysis
- Lesions after decussation – contralateral paralysis
(I) Pain and temperature – Lateral spinothalamic
- Receptors:
- Free nerve endings – pain
- Krause end bulb
- Ruffini’s corpsules
- 1st order neuron
- Dorsal root ganglion
- Spinal cord dorsal horn
- Synapse with 2nd order neuron in substantia gelatinosa
- Decussate in anterior white commisure
- Ascend as lateral spinothalamic tract
- And then as spinal lemniscus in medulla
- To VPLN of thalamus
- Synapse with 3rd order neuron
- Posterior limb internal capsule and corona radiata
- Posterior central gyrus
(II) Crude touch and pressure – Ventral spinothalamic
- Receptors:
- Paccinian corpuscle – pressure
- Merkel’s disc – mechanoreceptor
- 1st order neuron
- Dorsal root ganglion
- Spinal cord dorsal horn
- Synapse with 2nd order neuron in nucleus proprius
- Axons rise a few segments
- Decussate in anterior white commisure
- Ascend as anterior spinothalamic tract
- And then as spinal lemniscus in medulla
- To VPLN of thalamus
- Synapse with 3rd order neuron
- Posterior limb internal capsule and corona radiata
- Posterior central gyrus
(III) Concious proprioception, vibration and fine touch – Fasciculus gracilis and cuneatus
- Receptors:
- Paccinian corpuscle
- Muscle spindle
- Golgi tendon organ
- Meissner’s corpuscle – light touch
- 1st order neuron
- Dorsal root ganglion
- Ascend in ipsilateral fascicle
- Synapse with 2nd order neuron in medulla in nucleus gracilis/cuneatus
- Pyramidal decussation
- Ascend in medial lemniscus
- To VPLN of thalamus
- Synapse with 3rd order neuron
- Posterior limb internal capsule and corona radiata
- Posterior central gyrus
(IV) Unconcious proprioception/ reflex – From muscles to cerebellum
Ventral spinocerebeller
- Receptors:
- Muscle spindle
- Golgi tendon
- 1st order neuron
- Dorsal root ganglion
- Spinal cord dorsal horn
- Synapse with 2nd order neuron in dorsal horn
- Decussate in anterior white commisure
- Ascend as ventral spinocerebeller tract
- Enter cerebellum in superior cerebeller peduncle
- Decussate in cerebeller white mater
- Terminate in vermis
NB: No 3rd order neuron, 2 decussations
Dorsal spinocerebeller
- Receptors:
- Muscle spindle
- Golgi tendon
- 1st order neuron
- Dorsal root ganglion
- Spinal cord dorsal horn
- Synapse with 2nd order neuron in Clarke’s nucleus/ nucleus dorsalis
- Ascend ipsilateral in dorsal spinocerebeller tract
- Enter cerebellum in inferior cerebeller peduncle
- Terminate in vermis
NB: No 3rd order neuron, no decussations, ipsilateral tract
(V) Gustatory pathway – Taste
Descending pathways
- Upper motor and lower motor
Voluntary and fine movements

These are summarized notes from various sources, mainly TeachMeAnatomy and Wikipedia
Neuroanatomy and Cranial Nerves
Scalp
Extents:
- Superior nuchal line – posteriorly
- Supraorbital margins – anteriorly
- Zygomatic arch – lateral
Layers:

NB: Injury to scalp leads to prolonged bleeding due to rich blood supply and separation of vessel ends by connective tissue and aponeurosis. Also heals rapidly due to rich blood supply.
Nerves and arteries:

Venous:
- Supraorbital and supratrochlear drain into – facial vein
- Superficial temporal veins – retromandibular vein
- Posterior auricular veins – external jugular veins
- Occipital vein – vertebral veins
NB: The veins connect with intracranial sinuses through emissary veins (can spread infection)
Cranial meninges
3 layers of connective tissues that:
- Protect brain
- Provide framework for arteries and veins
- Enclose fluid filled cavity

(I) Dura mater:
Made of 2 layers that separate to form sinuses:
- Outer periosteal layer
- Inner meningeal layer
(II) Arachnoid mater:
- Avascular layer
- Attached to pia mater by web like arachnoid trabeculae
- Held against dura by pressure of CSF (cerebrospinal fluid)
(III) Subarachnoid space:
Contains arachnoid trabeculae, CSF, blood vessels and nerves
(IV) Pia mater:
- Vascularised
- Thin membrane that adheres to brain surface and follows its contours
- Prevents blood vessels coming in contact with neural tissue
Arterial supply to meninges:
- Middle meningeal artery
- Accessory meningeal artery
- 2 anterior meningeal arteries
- 2 posterior meningeal arteries
Clinicals:
- Epidural hemorrhage – injury to middle meningeal artery
- Subdural hemorrhage – superior saggital veins tear as they drain into superior saggital sinus
- Cerebral hemorrhage – middle cerebral artery branch ruptures
- Meningitis
Dural folds
Invagination of meningeal layer of dura mater – to compartmentalize and stabilize brain
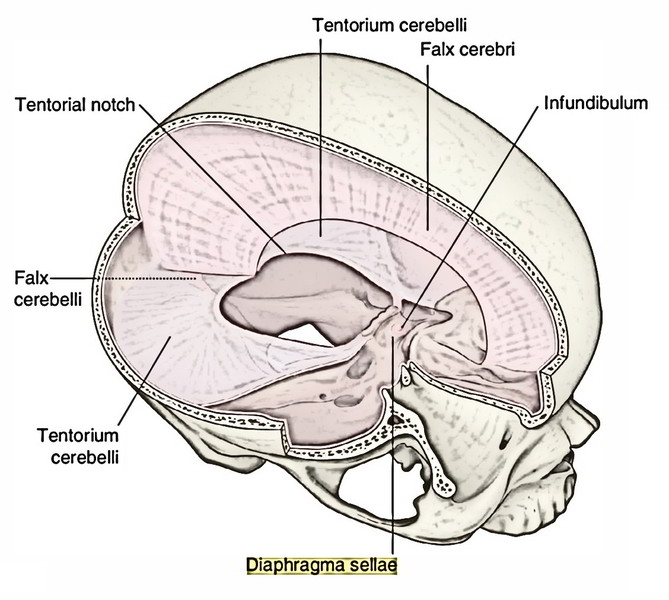

- Falx cerebri – Separate right and left cerebrum
- Falx cerebelli – Separate right and left cerebellum
- Tentorium cerebelli – Separates cerebellum and occipital lobes of cerebrum
- Diaphragm sellae – Roof of sella turica
Dural sinuses
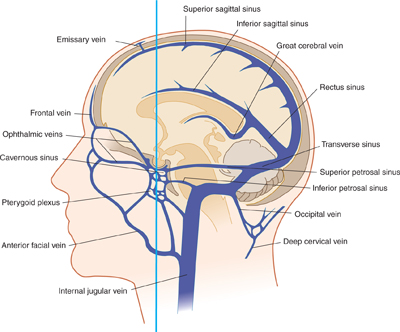
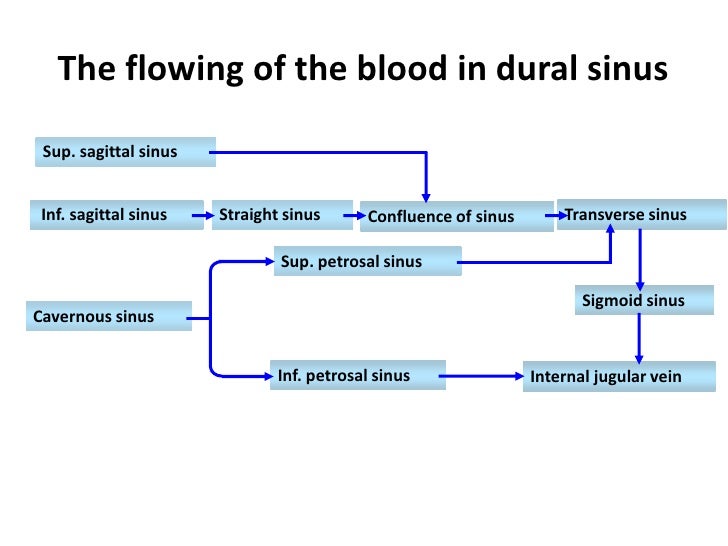
NB: Great cerebral vein joins inferior sagittal sinus to form straight sinus
Blood from superior sagittal sinus favours right transverse sinus
The skull
3 components:
- Neurocranium/ calvaria
- Chondrocranium/ skull base
- Vicerocranium/ facial skeleton
Neurocranium:

Chondrocranium:

Vicerocranium:
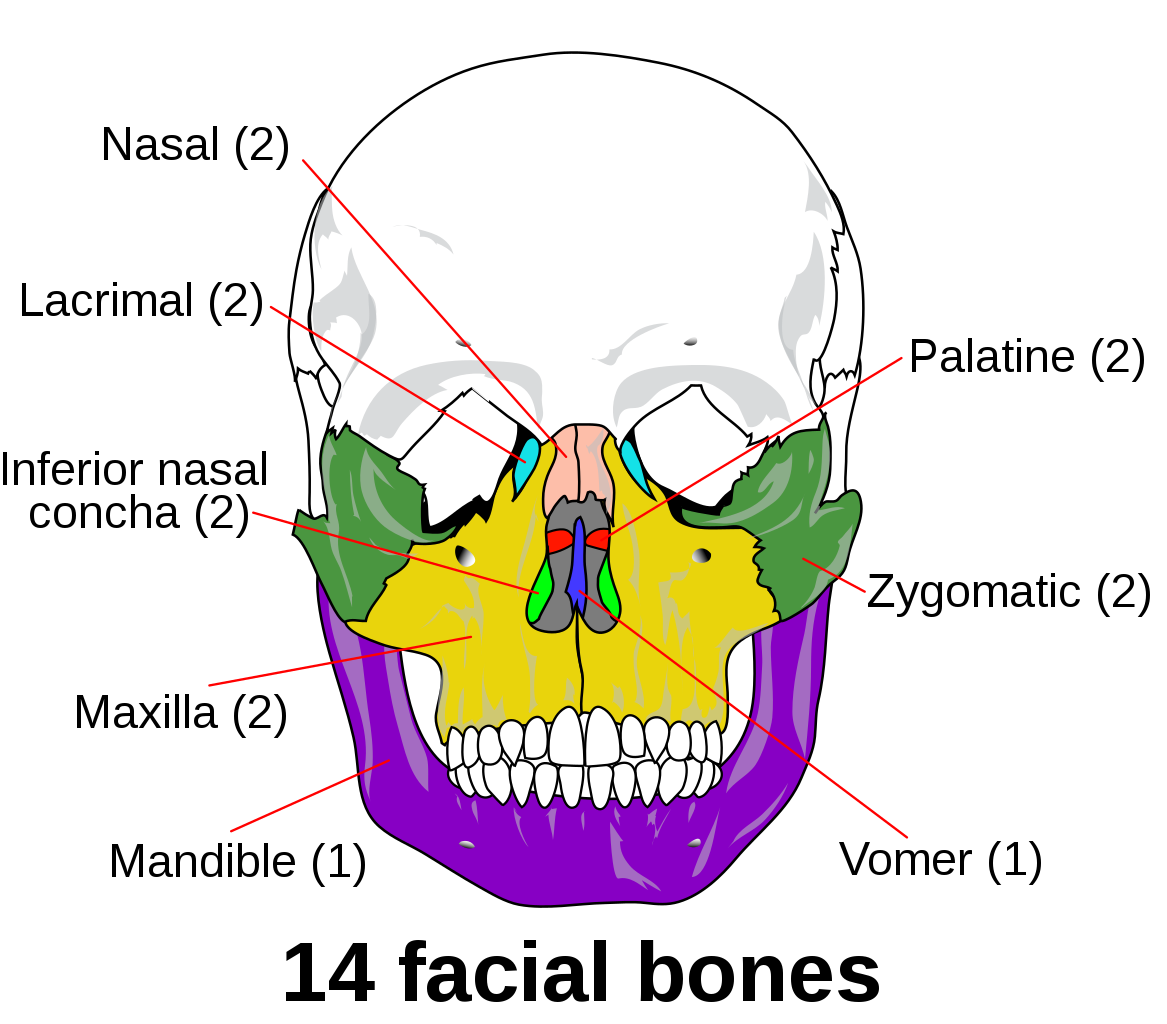
Sutures of skull

Difference between adult and neonate skull:
1. Ratio of vicerocranium : neurocranium
- Neonate 1:8
- Adult 3:8
2. In neonate, has fontanelles which close:
- Posterior – 3 months after birth
- Sphenoid – 6 months
- Mastoid – 18 months
- Anterior – 18-24 months
3. Neonate does not have all air sinuses
4. Neonate has less prominent mastoid
5. Neonate angle of mandible more obtuse
6. Neonate has no alveolar process
7. Neonate has no styloid process
8. Neonate basal skull ossifies after birth
9. Neonate has no diploe – to enable bone molding during birth
10. Neonate has metopic/frontal suture which disappears after 2 years
Functions of sutures:
- Allow for birth
- Molding and brain growth
- Age estimation
- Draw CSF and blood from fontanelles
Clinicals:
1. Pterion – Thin and weak, made of Frontal, parietal, squamous temporal and greater wing sphenoid. Overlies middle meningeal artery (anterior division). Therefore fracture can damage the artery and lead to epidural hematoma
2. Raised intracranial pressure – bulges anterior fontanelle
3. Sunk anterior fontanelle – dehydration due to diarrhea and vomit
4. Hydrocephaly: Accumulation of CSF, widening spaces called ventricles
- Communicating – CSF no reabsorbed but can flow from ventricle to ventricle
- Non communicating – Obstruction in flowing from one ventricle to another

Cranial fossa
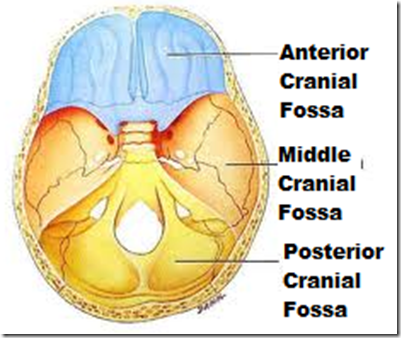
(I) Anterior cranial fossa
Borders:
- Anterior – Frontal bone
- Posterior – Lesser wing sphenoid
- Medial – Cribriform plate
- Lateral – Orbital of frontal bone
- Floor – All of the above
Contents: Frontal lobe, olfactory bulb and tract
Clinicals: Cribriform fracture: loss of smell, CSF in nasal
(II) Middle cranial fossa
Borders:
- Anterior – Lesser wing sphenoid
- Posterior – Petrous temporal
- Medial – Greater wing shenoid
- Lateral – Squamous temporal and parietal bone
- Floor – Sella turcica and greater wing sphenoid
Contents: Temporal lobes, cavernous sinus, pituitary gland, optic chiasma
Clinicals: Pituitary surgery
(III) Posterior cranial fossa
Borders:
- Anterior – Dorsum sellae, petrous temporal
- Posterior – Squamous occipital
- Medial – Dorsum sellae
- Lateral – Mastoid temporal
- Floor – Tentorium cerebelli and occipital bone
Contents: Cerebellum, pons, medulla
Clinicals: Cerebellum tonsillar herniation via foramen magnum
Skull foramina and contents
1. Foramen cecum: Emissary veins (nasal to superior sagittal sinus)
2. Cribriform foramina: Olfactory nerve (CN 1) – nasal to olfactory bulb
3. Optic canal:
- Optic nerve (CN 2) – surrounded with meninges
- Opthalmic artery branch – lacrimal artery
4. Superior orbital fissure:
- Oculomotor nerve (CN 3)
- Trochlear nerve (CN 4)
- Abducens nerve (CN 6)
- Opthalmic nerve (CN 5-1)
- Superior opthalmic vein
5. Foramen rotundum: Maxillary nerve (CN 5-2)
6. Foramen ovale: MALE
- Mandibular nerve (CN 5-3)
- Accessory meningeal artery
- Lesser petrosal nerve
- Emissary veins (pterygoid plexus – cavernous sinus)
7. Foramen lacerum:
- Greater petrosal nerve
- Internal carotid artery
8. Foramen spinosum:
- Middle meningeal artery
- Middle meningeal vein
- Nervous spinosus (nerve branch of 5-3)
9. Carotid canal: Internal carotid artery
10. Internal acoustic meatus:
- Facial nerve (CN 7)
- Vestibulocochlear nerve (CN 8)
- Labyrinthine artery
11. Jugular foramen:
- Glossopharyngeal nerve (CN 9)
- Vagus nerve (CN 10)
- Accessory nerve (CN 11)
- Inferior petrosal sinus
- Sigmoid sinus
- Posterior meningeal artery
12. Mastoid foramen:
- Facial nerve (CN 7)
- Emissary veins
13. Hypoglossal canal: Hypoglossal nerve (CN 12)
14. Foramen magnum:
- Medulla
- Meninges
- Vertebral arteries
- Spinal arteries

15. Supraorbital foramen: Supraorbital nerve (from frontal nerve from opthalmic nerve 5-1)
16. Infraorbital foramen: Infraorbital nerve of 5-2
17. Mental foramen: Mental nerve
Cranial nerves
- Olfactory – Sensory
- Optic – Sensory
- Oculomotor – Motor
- Trochlear – Motor
- Trigeminal – Both
- Abducens – Motor
- Facial – Both
- Vestibulocochlear – Sensory
- Glossopharyngeal – Both
- Vagus – Both
- Accessory – Motor
- Hypoglossal – Motor
Mnemonic: Oh Oh Oh To Touch And Feel Very Good Velvet Ah Heaven!
Mnemonic: Some Say Marry Money But My Brother Says Big Brains Matter Most
Cranial nerve courses
NB: Summarised notes made from: Teachmeanatomy
(I) Olfactory nerve: Special Viceral Afferent (smell)
- Olfactory mucosa containing non myelinated axons
- Axons bundle to form a bundle – filia olfactoria
- Pass through cribriform plate foramina
- Enter olfactory bulb
- Olfactory nerves synapse with mitral cells
- Forming a synaptic glomeruli
- The mitral cells run posteriorly in the olfactory tract
- At the anterior perforated substance, tract divides into medial and lateral stria
- Lateral stria axons go to primary olfactory cortex – piriform region
- Medial stria carry axons across anterior commissure to opposite olfactory bulb
Clinicals:
- Anosmia – loss of sense of smell (cribriform plate fracture/ meningitis etc.)
- Olfactory hallucinations – detect smells which are not present (tumor/ Parkinson’s disease)
(II) Optic nerve: Special Somatic Afferent
- NB: covered by oligodendrocytes (not schwaan cells) and meninges
- Receptor: Rods and cones
- 1st order: Bipolar cells
- 2nd order: Ganglion cells
- Many ganglion cells inside tendinous ring pass through optic canal
- Optic nerves meet at optic chiasma at pituitary gland
- Which forms optic tract
- Goes to lateral geniculate body of thalamus
- 3rd order neuron from optic radiation to primary visual cortex
Regions where optic tract is projected:
- Lateral geniculate body
- Superior colliculus
- Pretectal nucleus
- Suprachiasmatic nucleus
Visual fields:

(III) Oculomotor nerve: General Sympathetic Efferent (eye movement) and General Viceral Efferent (parasympathetic – constriction of pupil)
(A) GSE
- From oculomotor nucleus
- Through red nucleus
- Through substantia nigra
- Exits through interpeduncular fossa
- Pierces dura mater
- Through lateral wall of cavernous sinus
- Through superior orbital fissure
- And divides into:
- Superior branch – levator palpebrae superioris and superior rectus muscles
- Inferior branch – medial rectus, inferior rectus, inferior oblique muscles
(B) GVE
- From Edinger-Westphal nucleus
- Travel in inferior branch
- To ciliary ganglion (synapse)
- Post ganglionic, short ciliary nerves pierce sclera
- Innervates:
- Spincter pupillae – smooth muscles of iris, constrict pupil
- Ciliary muscle – tighten/relax lens
Clinicals: Oculomotor nerve lesions due to:
- Increased intracranial pressure
- Aneurysm of posterior cerebral artery
- Cavernous sinus infection or trauma
Results in:
- External strabismus – eyeball down and lateral
- Ptosis – drooping upper eyelid
- Dilated pupil
(IV) Trochlear nerve: GSE (Superior oblique muscle)
- From trochlear nucleus, emerging from posterior midbrain
- Winds around brainstem
- Pierce dura of tentorium cerebelli
- Through lateral wall of cavernous sinus
- Through superior orbital fissure
- Enter orbit of eye
- Innervates superior oblique muscle
Clinicals: Trochlear paralysis – caused by vascular lesions, cavernous thrombosis, hypertension, diabetes mellitus etc.
Results in:
- Verticle diplopia – double vision
- External strabismus
(V) Trigeminal nerve: GSA and SVE
Nuclei:
- Mesenocephalic nucleus – sensory (proprioception)
- Main sensory – sensory (touch)
- Spinal nucleus – sensory (pain and temperature)
- Motor nucleus of trigeminal – motor (muscles of mastication)


Course:
- Emerges from lateral aspect of pons
- Forms trigeminal ganglion and splits into 3 branches:
V1 – Opthalmic – GSA
- Pierces dura mater
- Passes through lateral wall of cavernous sinus and superior orbital fissure
- Branches:
- Lacrimal
- Frontal (supratrochlear and supraorbital through supraorbital foramen)
- Nasociliary (short ciliary, long ciliary, infratrochlear, anterior and posterior ethmoidal)
V2 – Maxillary – GSA
- Through lateral wall of cavernous sinus and foramen rotundum
- Enters pterygopalatine fossa
- Exits via inferior orbital fissure
- Through inferior orbital groove and canal
- Exits through infra orbital foramen
- Branches:
- Meningeal
- Infraorbital (inferior palpebral, nasal and superior labial)
- Zygomatic
- Anterior, middle and posterior superior alveolar
- Pterygopalatine nerves
V3 – Mandibular – GSA, SVE
- Joins motor nerve
- Through foramen ovale
- In infratemporal fossa
Innervation:

Clinicals:
- Paralysis of muscles of mastication – due to trauma, tumor, aneurysm, meningitis, polio, multiple sclerosis, vascular lesions. Jaw deviates to side of lesion.
- Loss of sensation of soft touch, thermal and pain in face
- Loss of cornea and sneezing reflex
- Herpes zoster
(VI) Abducens nerve – GSE (lateral rectus muscle)
- Abducens nuclei
- Emerges from the ponto medullary junction
- Through cavernous sinus (medially)
- Through superior orbital fissure and common tendinous ring
- To orbit of eye
- Innervates lateral rectus – abducts eye
Clinicals: Abducens nerve lesion due to basilar or internal carotid artery aneurysms, cavernous thrombosis
Results in:
- Internal strabismus – eye down and towards nose
- Diplopia
(VII) Facial nerve: GVA, GVE, GSA, SVA, SVE
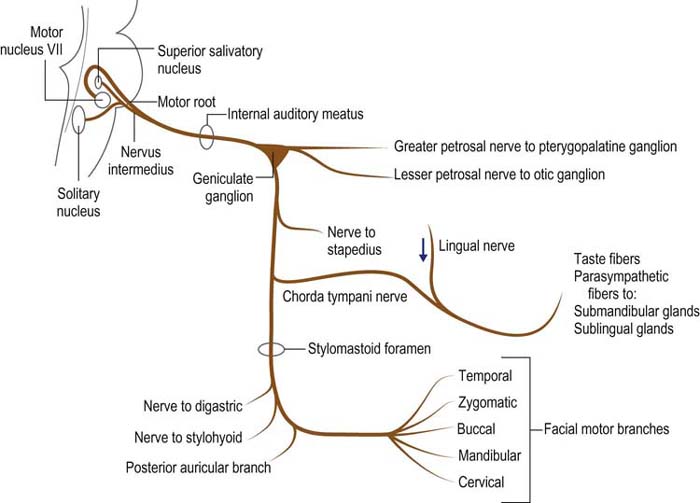
- Facial nerve is made of a motor root and intermediate nerve
- Both exit through cerebellopontine angle and internal auditory meatus
- Intermediate nerve synapses in geniculate ganglion (motor root does not)
- Both go through facial canal
- After exiting facial canal, intermediate nerve splits into:
- Greater petrosal nerve
- Chorda tympani (exits via pterygotympanic fissure)
- Motor nerve gives nerve to stapedius
- Then exits through mastoid foramen
- Gives off 3 other nerves: Posterior auricular, nerve to posterior belly diagastric and stylohyoid
- Pierces body of parotid gland and gives off the facial motor branches
Clinicals:
- Paralysis of facial nerve – ipsilateral paralysis of facial muscles
- Bells palsy

- Loss of taste – Chorda tympani, anterior 2/3 tongue
- Ipsilateral hyperacusis
- Decrease in gland production – lacrimal, sublingual, submandibular. Leads to dry eyes and dry mouth
(VIII) Vestibulocochlear nerve: SSA
- From vestibulocochlear nuclei
- Emerges from cerebellopontine angle
- Through internal acoustic meatus
- Divides into:
- Vestibular division ⇒ vestibular ganglion ⇒ hair cells etc.
- Cochlear division ⇒ spiral ganglion ⇒ spiral organ
NB: Vestibulo ocular reflex – allow images on retina to stabilize when head turns by moving eyes in opposite direction

Clinicals:
- Vestibular neuritis – inflammed vestibular nerve division. Results in vertigo, nausea, posture imbalance
- Labyrinthitis – inflammed membranous labyrinth, results in hearing loss, tinnitus (false ringing sound)
(IX) Glossopharyngeal nerve: GVA, GVE, GSA, SVA, SVE
Nuclei:

Course:
- Emerges from lateral medulla
- Leaves via jugular foramen
- Outside foramen are superior and inferior ganglia (contain cell bodies of sensory fibers)
- Branches:
- Nerve to stylopharyngeus
- Carotid sinus
- Pharyngeal branch – oropharynx mucosa
- Tonsilar branch – palatine tonsils
- Lingual branch – general and taste sensation in posterior 1/3 tongue
- Tympanic nerve ⇒ Becomes lesser petrosal nerve ⇒ Through foramen ovale ⇒ Synapse at otic ganglion which supplies to parotid gland (salivary secretion and vasodilation)
Clinicals:
- Loss of gag reflex
- Loss of taste in ipsilateral posterior 1/3 tongue
- Reduced parotid secretion – ipsilateral
- Ipsilateral weakess in swallowing
- Glossopharyngeal neuralgia – pain when swallowing or talking
(X) Vagus nerve: GVA, GVE, GSA, SVA, SVE
NB: Longest CN
Nuclei:

Course:
- Emerges from medulla of brainstem
- Gives out auricular branch (innervates external ear and external auditory canal)
- Goes through jugular foramen
- Through carotid sheath with internal jugular vein and common carotid artery
- Posterior to sternoclavicular joint, enter thorax
Branches in neck:
- Pharyngeal branches – motor to pharynx and soft palate muscle (except tensor palatine)
- Internal laryngeal nerve – Sensory to superior pharynx
- External laryngeal nerve – cricothyroid muscle
- Right recurrent laryngeal nerve – intrinsic larynx muscles
In thorax:
- Right vagus nerve forms posterior vagal trunk
- Left forms anterior vagal trunk
- Branches:
- Left recurrent laryngeal nerve – intrinsic larynx muscles
- Cardiac branches
- Contribute to oesophageal plexus
In abdomen:
- Vagal trunks enter abdomen via oesophageal hiatus in diaphragm
- In abdomen terminate by dividing into branches that supply: esophagus, stomach, small and large bowel, anterior and posterior gastric, celiac ganglion, superior mesenteric ganglion, splenic and gastric branches, pancreatic and pyloric branches, and to small and large intestines
NB: Palatoglossus innervated by vagus nerve
Clinicals:
Injury by aneurysm, cerebellopontine angle lesions, hydrocephalus, tumors, vascular lesions of brainstem
Results in:
- Dysphonia – difficulty in speaking
- Dysphagia – difficulty in swallowing
- Loss of gag reflex
- Deviation of uvula
- Hyperacidity
- Gastric ulcers
(XI) Spinal accessory nerve: SVE (sternocleidomastoid and trapezius muscle)
- Nerve from spinal accessory nucleus
- Goes through foramen magnum
- Joins with nerve from nucleus ambiguus
- Together exit jugular foramen
- Splits to innervate trapezius and sternocleidomastoid muscles
Clinicals:
- Drooping shoulders
- Assymetrical neck line
- Can’t rotate head down and away
(XII) Hypoglossal nerve: GSE (tongue muscles except palatoglossus)
- From hypoglossal nucleus
- Emerges from medulla oblongata between olive and pyramid
- Exits via hypoglossal canal
- Passes inferior to angle of mandible
- Crosses internal and external carotid arteries
- Enters tongue
Clinicals: Deviated tongue – ipsilateral
Spinal cord
Parts:
Extents: Foramen magnum to L1/L2 in adults, L3 in infants
Enlargements: Cervical (C4-T1), Lumbosacral (L2-S3)
Blood supply:
- 1 anterior spinal artery – anterior 2/3 of spinal cord
- 2 posterior spinal arteries – posterior 1/3 of spinal cord
- Radicular arteries – from ascending cervical, inferior thyroid, intercostal, lumbar and sacral arteries


Spinal veins:
- Drain into internal vertebral venous plexus (epidural)
- Which consists of anterior and posterior longitudinal venous channels – made of 6 longitudinal veins
- Also connect with external venous plexus
- Connect intracranial sinuses to superior vena cava

Contents of intervertebral foramen: Spinal nerve, dorsal root ganglion, radicular vessels, associated sympathetic plexus
Support: Spinal nerves, continuation of brain stem, denticulate ligaments (pia mater to dura mater)
Protection: Vertebral column bones, spinal meninges, CSF
Spinal nerves:
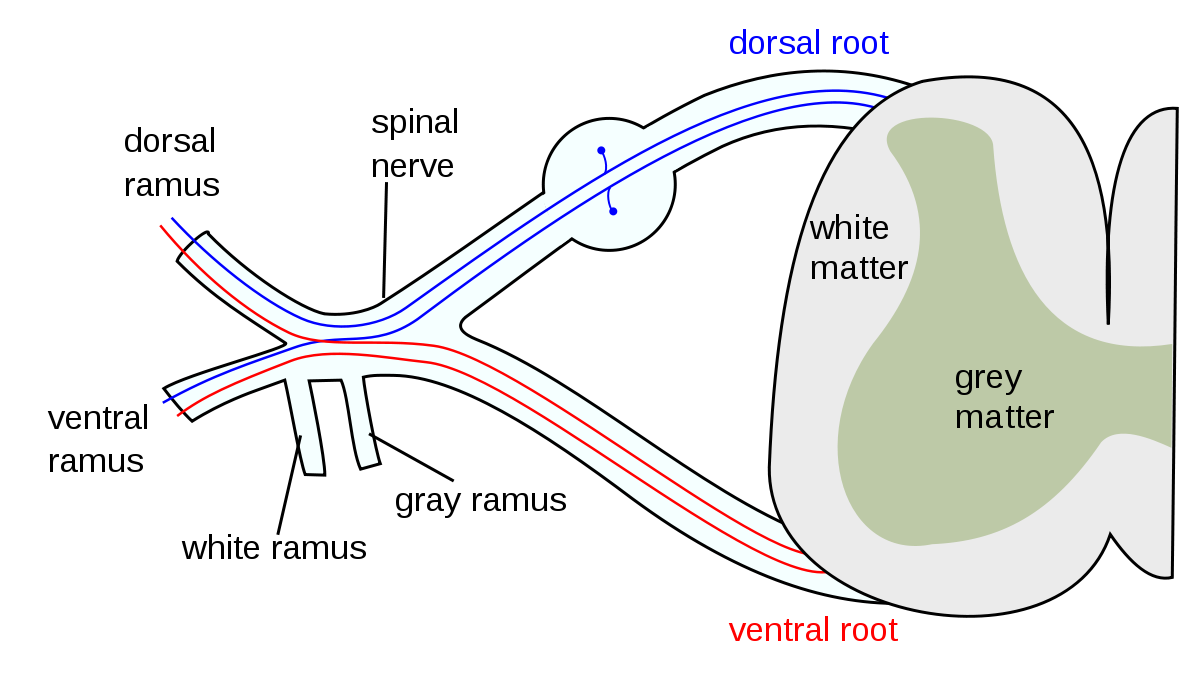
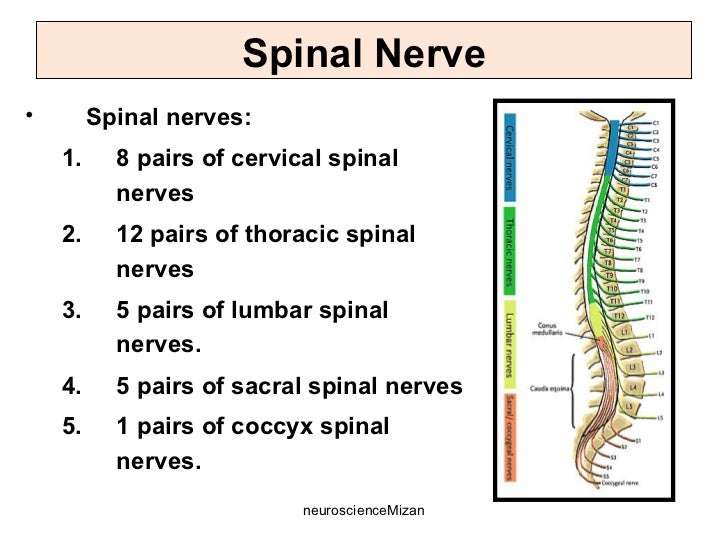
- From C1-C7, spinal nerves exit above respective vertebra
- C8 spinal nerve exits below C7 vertebra
- From T1 onwards, spinal nerves exit below their respective vertebra
- Conus medullaris – Cone shaped end of spinal cord
- Cauda equina – Nerve roots after spinal cord has ended

Dermatomes:

Spinal tracts: (Tractology in next chapter)
(I) Ascending tracts – afferent nerves
1st order – Dorsal root ganglion
- General sensation (psuedounipolar neuron) – pain, temperature, touch, pressure, vibration and proprioception
- Special sensation (bipolar neuron) – hear, vision, taste, smell, balance
2nd order:
- Synapse with 1st order in spinal cord
- Cross over
- Terminate in thalamus
3rd order:
- Synapse with 2nd order in thalamus
- Terminate in cortex
(II) Descending tracts – efferent nerves
- Upper motor – From brain to anterior horn of brainstem/spinal cord
- Lower motor – From anterior horn of brainstem/spinal cord to effectors
Spinal segments:
Clinicals:
- Central cord syndrome:

2. Anterior cord syndrome:

3. Posterior cord syndrome:

4. Brown sequard syndrome:
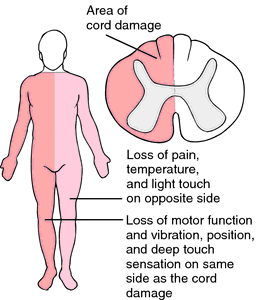
5. Chicken pox – virus can travel through sensory axons of single dermatome and erupt onto skin in a single dermatome – known as Herpes zoster/Shingles (reactivation of latet chicken pox)
6. Quadriplegia – damage below C3; paralysis of whole trunk, arms and legs
7. Paraplegia – damage to middle spinal cord T1-L4; paralysis to legs and part of trunk
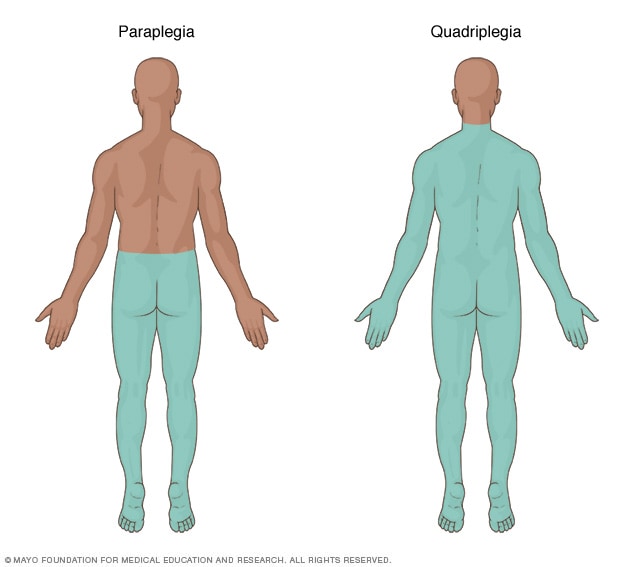
8. Lumbar cistern:
- Subarachnoid space at L3-L4 after spinal cord terminates
- Site for lumbar puncture – Patient curls so spinous process spaced. Drain CSF to diagnose meningitis.
- Pierces skin ⇒ subcutaneous tissue ⇒ thoracolumbar fascia ⇒ supraspinous ligament ⇒ interspinous ligament ⇒ epidural space ⇒ dura mater ⇒ subdural space ⇒ arachnoid mater

Cerebrum
Deep median longitudinal fissure – separates the 2 hemispheres
The main sulci – Central and lateral, divide cerebrum into frontal, parietal, temporal and occipital lobes
1. Frontal lobe
From central sulcus to frontal pole, from longitudinal median fissure to lateral sulcus
4 principle gyri:
- Precentral gyrus
- Superior frontal gyrus
- Middle frontal gyrus
- Inferior frontal gyrus
The lateral sulcus divides inferior frontal gyrus into:
- Pars orbitale
- Pars triangularis
- Pars opercularis
Olfactory tract divides into:
- Lateral olfactory stria
- Medial olfactory stria
2. Parietal lobe
Is divided into:
- Superior parietal lobule – somatosensory association
- Inferior parietal lobule – consists of supramarginal gyrus and angular gyrus
NB: Lower part of supramarginal gyrus forms Wernicke’s area (sensory speech)
3. Temporal lobe
On the outer bank of lateral sulcus is transverse gyri of Heschl (primary auditory area)
4. Occipital lobe
Contains primary and secondary visual cortex on either side of calcarine sulcus


Functional areas of brain:
- Primary motor area – Precentral gyrus (somatic motor activity)
- Premotor area – Plans motor activity
- Prefrontal area – High CNS function (intelligence, memory, reasoning)
- Broca’s area – Motor speech (pars opercularis + pars triangularis) – if you are right handed, it is found on the left hemisphere and vice versa
- Primary sensory area – Post central gyrus (awareness of sensation)
- Wernicke’s area – Sensory or understanding speech (supramarginal gyrus)
- Primary auditory area – Transverse gyri of Heschl in superior temporal gyrus (awareness of sound)
- Secondary auditory area – Superior temporal gyrus
- Primary visual area – Both banks of calcarine sulcus
- Secondary visual area
- Olfactory area – uncus (for smell)
- Gustatory area – Taste (shown in diagram)
- Horizontal eye movement – Middle frontal gyrus, middle part
Circle of Willis:
- Internal carotid artery
- Vertebral artery

Cerebrum blood supply:
(I) Anterior cerebral artery:

- Runs in callosal sulcus
- Supplies medial surface of cerebrum
Clinicals:
- Contralateral hemiplegia – Paracentral lobule: Motor and sensory loss of lower limbs
- Apraxia – Corpus callosum: Difficulty in doing tasks or learned movements
- Agnosia – Loss of sensation
- Hemihyperacusis – Increase sensitivity to sound
(II) Middle cerebral artery:
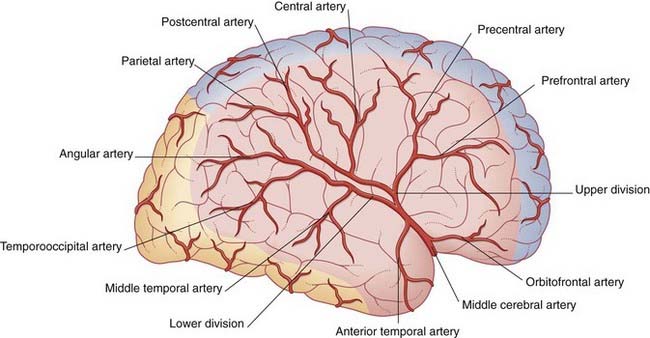
- Runs in lateral sulcus
- Supplies lateral surface of cerebrum
Clinicals:
- Contralateral loss of discriminating touch
- Contralateral hemiplegia – Motor and sensory loss of upper extremity and face
- Global aphasia – Broca’s area, Motor speech lost
- Partial deafness – Superior temporal gyrus
(III) Posterior cerebral artery:
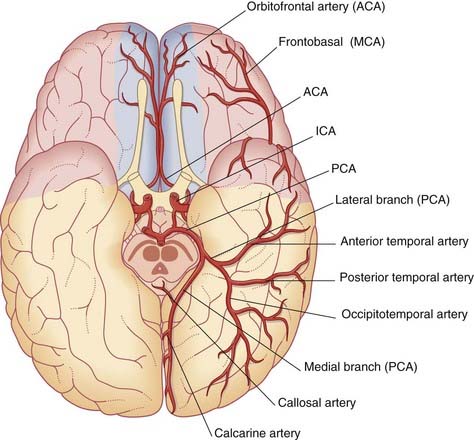
- Supplies occipital lobe, midbrain, brainstem, choroid plexus and visual cortex
Clinicals:
- Blindness
- Tunneling of vision
- Superior alternating hemiplegia/ Weber’s syndrome
Cerebral veins:
(I) Superficial cerebral veins: Run in subarachnoid space

- Superior cerebral veins – drain into superior sagittal sinus
- Superficial middle cerebral vein (runs in lateral sulcus) – drains into cavernous sinus
Also divides into:
- Superior anastomotic vein – drains into superior sagittal sinus
- Inferior anastomotic vein – drains into transverse sinus
3. Inferior cerebral vein – drains into cavernous and transverse sinus
(II) Deep cerebral veins
Basal veins (paired) and internal cerebral veins (paired) drain into great cerebral vein

Clinicals:
- Agnosia – can’t interpret sensation or recognize things
- Hemineglect – not aware of one side of body
- Visual agnosia – can’t interpret visual information
- Prosopagnosia – can’t recognize familiar faces or recall visual memories
- Apraxia – unable to perform tasks or learned movements
- Aphasia – can’t understand or express speech
- Alexia – can’t read
- Dyslexia – inability to read more than a few lines with understanding
Brain stem
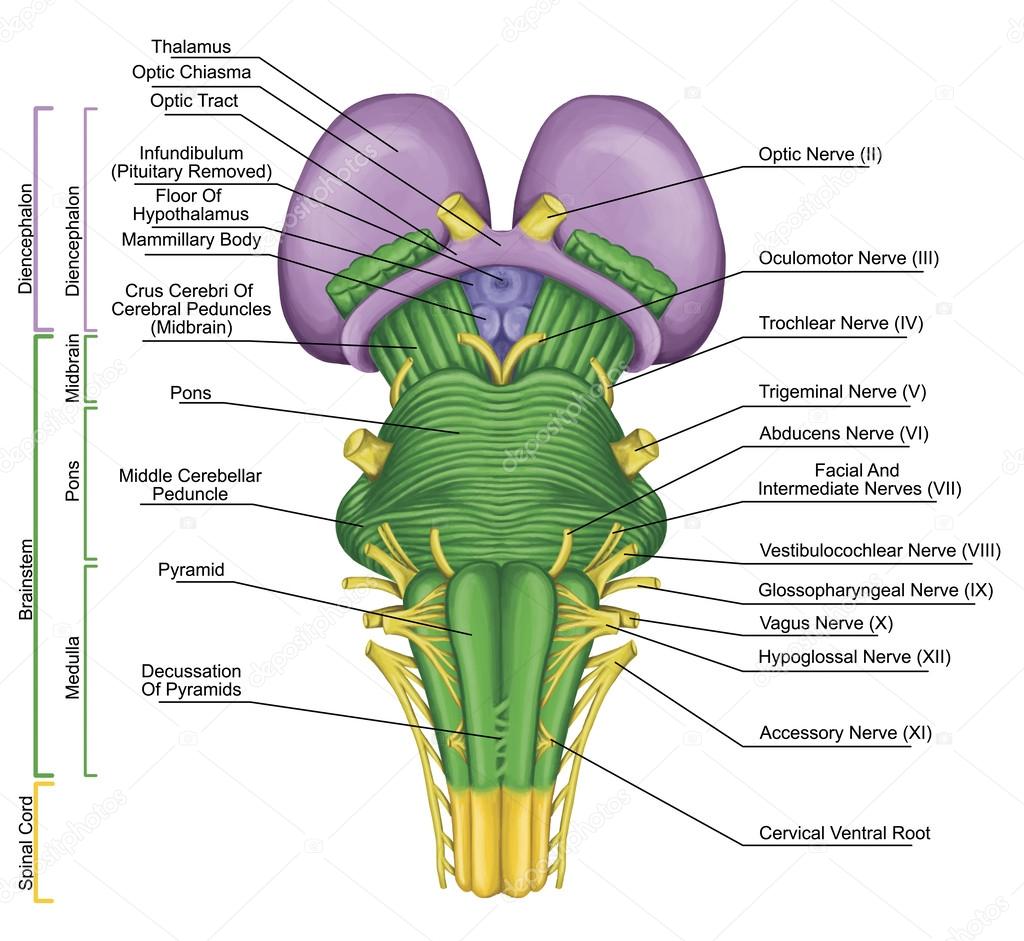
Nuclei of brain stem:

Vascular lesions of:
(I) Midbrain – Superior alternating hemiplegia/Weber’s syndrome
Occlusion of mesencephalic branch of posterior cerebral artery
- Pyramidal fibers – contralateral hemiparesis
- Occulomotor nerve – ipsilateral paralysis of occular muscles except lateral rectus and superior oblique muscles
(II) Pons – Middle alternating hemiplegia
Occlusion of pontine branches
- Corticospinal fibers – contralateral hemiparesis
- Abducens nerve – ipsilateral paralysis of lateral rectus muscle
(III) Medulla – Inferior alternating hemiplegia
A) Medial medullary syndrome
Occlusion of medullary branch of anterior spinal artery/bulbar branch of vertebral artery
- Medial lemniscus – contralateral loss of discriminating touch, vibration, position and movement sensations
- Hypoglossal nerve – ipsilateral tongue paralysis
B) Lateral medullary syndrome/ Wellenbergs syndrome
Occlusion of medullary branch of posterior inferior cerebeller artery
- Spinal lemniscus – Contralateral loss of pain and temperature
- Nucleus ambiguus – ipsilateral palate muscle paralysis in swallowing and phonation
- Trigeminal nerve – ipsilateral loss of pain and temperature on face
Cerebellum
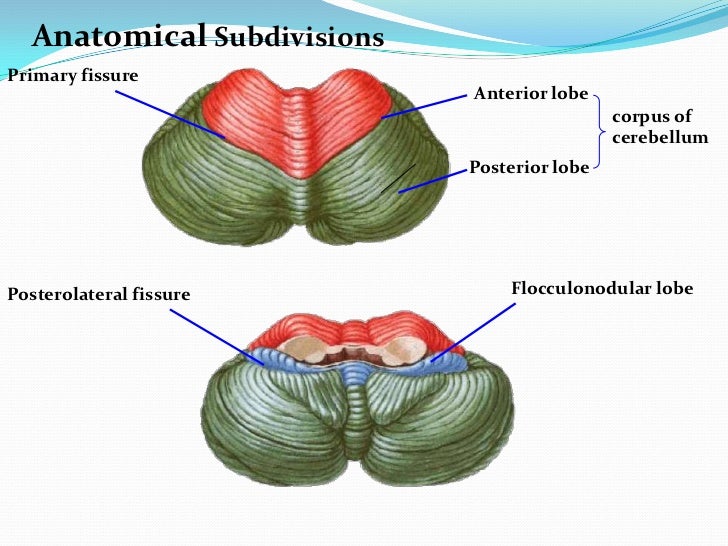

Blood supply:
- Posterior inferior cerebeller artery (PICA)
- Anterior inferior cerebeller artery (AICA)
- Superior cerebeller artery (SCA)
Vein: Great cerebral vein
Nuclei:

Cerebeller peduncles:
- Superior – Midbrain
- Middle – Pons
- Inferior – Medulla
Others
1. Cerebellopontine angle:

Contents:
- Facial nerve
- Vestibulocochlear nerve
- Labyrinthine artery
Clinicals: Cerebellopontine tumor – compress nerves, cerebellum and pyramids
2. Interpeduncular fossa:

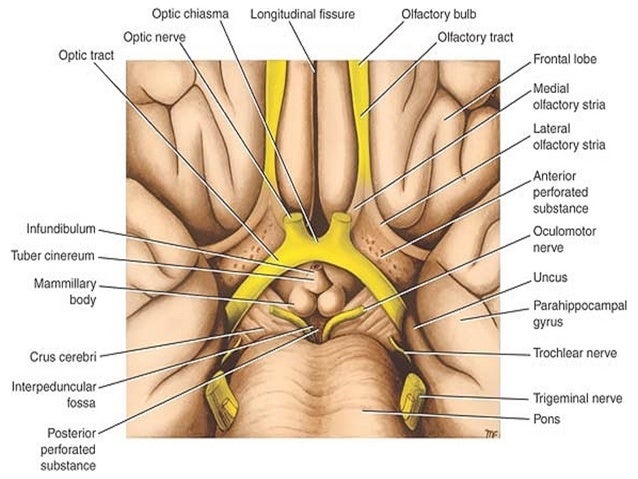
Contents:
- Mammillary bodies
- Occulomotor nerve
- Infundibulum stalk
- Tuber cinereum
- Posterior perforated substance
Clinicals: Tumors – compress nerves, hypothalamus and crus cerebri
3. Pineal body:
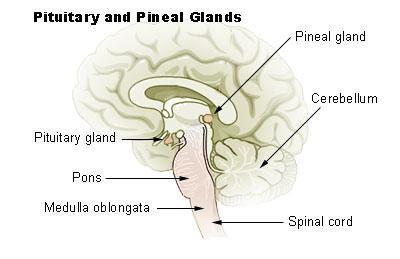
Relations:
- Laterally – Cerebral hemispheres (thalamic bodies)
- Rostrally: Wall of 3rd ventricle
- Inferiorly: Superior colliculus
Functions:
- Produce melatonin
- Regulate circadian rhythm
- Modulation of sleep patterns
- Delays puberty
- Neuroendocrine transducer
Clinicals:
- Vertical gaze palsy – can’t move eyes up, pineal gland tumor
- Pseudopuberty precocious
4. Corpus callosum

Blood supply:
- Pericallosal artery
- Subcallosal artery
- Median callosal artery
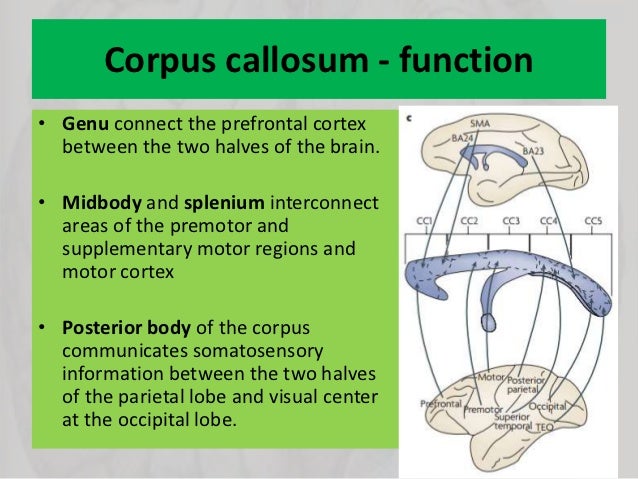
5. Commissural fibers:
Connect the 2 hemispheres of the brain:

6. Association fibers:


7. Cavernous sinus:


Relations:
- Superior – Temporal lobe
- Inferior – Sphenoid air sinus
- Medial – Pituitary gland
- Lateral – Trigeminal ganglion
- Anterior – Optic nerve
- Posterior – Petrous temporal bone
Contents: Internal carotid artery, CN 3, 4, 5-1, 5-2, 6
Clinical: Spread of infection, cavernous sinus thrombosis
NB: Drains in pterygoid plexus
8. Pituitary gland:
Location: On sella turcica
Relations:
- Superior – Optic chiasma
- Inferior – Sphenoid air sinus
- Lateral – Cavernous sinus
- Anterior – Spenoid air sinus
- Posterior – Dorsum sellae
Clinical: Pituitary tumor – endocrine dysfunction
9. Diencephalon:

(I) Thalamus:
Relations:
- Superior – Floor of lateral ventricle
- Inferior – Hypothalamus
- Medial – 3rd ventricle
- Lateral – Internal capsule
Blood supply: Posterior communicating, posterior cerebral, anterior choroidal
Nuclei:

(II) Hypothalamus:
Relations:
- Superior – Thalamus
- Inferior – Optic chiasma
- Anterior – Frontal lobe
- Posterior – Midbrain
- Lateral – Internal capsule
- Medial – 3rd ventricle
10. CSF and ventricular system:

Production and flow of CSF:
- Choroid plexus in lateral ventricle produces CSF
- Flows in 3rd ventricle via intraventricular foramina
- To 4th ventricle via cerebral aqueduct
- Flows into subarachnoid space over brain and spinal cord vis paired lateral foramina of Lushka and median foramen of Magendi
- Resorption into venous sinus by arachnoid granulations in superior sagittal sinus
- Flows by pulsation of spinal arteries
Functions of CSF:
- Cushion brain
- Support brain weight
- Provide nutrients, remove waste
- Integration of endocrine functions
11. Basal ganglia: Deep nuclei of cerebrum which regulate motor activity
- Caudate nucleus
- Putamen
- Globus pallidus – Medial and Lateral
- Subthalamic nucleus
- Substantia nigra
- Striatum: Caudate nucleus and putamen
- Lentiform nucleus: Putamen and globus pallidus
12. Horizontal cross section of cerebrum:

13. Papez circuit of emotions:

These are summarized notes from various sources, mainly TeachMeAnatomy and Wikipedia
Anatomy of Upper Limbs
Bones and how to side them
Vertebra:
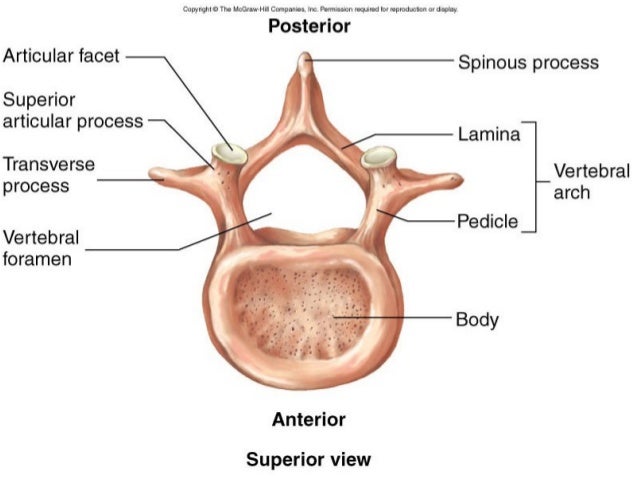
Types of vertebra:

Atlas (C1) – no body, no spinous process, dens foramen, transverse foramen, anterior and posterior arch and tubercle
Axis (C2) – dens, bifid spine, transverse foramen
Cervical vertebra – bifid spine (C7 is long and not bifid), transverse foramen and horizontal articular facets
Thoracic vertebra – vertical articular facets, heart shaped body, spine long and downwards
Lumbar vertebra – sagittal articular facets, kidney shaped body

Vertebral ligaments:
- Anterior longitudinal – prevent hyper extension
- Posterior longitudinal – prevent hyper flexion
- Ligamentum flavum – prevent abrupt flexion (between laminas)
- Interspinous
- Supraspinous
- Intertransverse ligament

- Static stability of vertebral column – ligaments
- Dynamic – back muscles ie. iliocostalis, longissimus, spinalis (from lateral to medial)
NB: Vertebral column divided into 3 vertical parallel columns:

Anterior column:
- Anterior longitudinal ligament
- Anterior 2/3 of vertebral body
- Anterior 2/3 of intervertebral disc (annulus fibrosus)
Middle column:
- Posterior 1/3 of vertebral body
- Posterior 1/3 on intervertebral disc
- Posterior longitudinal ligament
Posterior column:
- Ligament flavum
- Pedicles
- Facet joints and articular processes
Scapula:
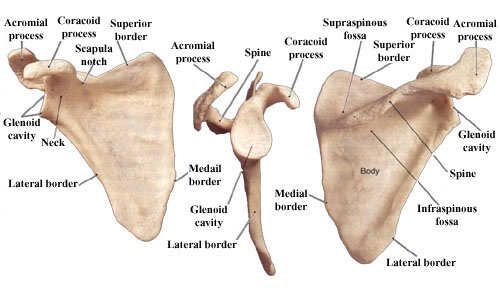
Clavicle:
- Acromial/lateral end is flat
- Sternal/medial end is thick and round
- Superior surface is smooth, inferior surface is rough
- Medial curve protrudes outward

Unique features of clavicle:
- Ossifies during week 5 (fetal) and completed at 25 years, others ossify at week 8 and complete at 18-21 years
- Runs a sigmoid, horizontal course
- No marrow cavity, core occupied by spongy bone
- Medial 2/3 ossify endochondrally, lateral 1/3 intramembranously
Functions of clavicle:
- Hold upper limb away from trunk and increase range of movement such as abduction
- Transmit weight from upper limbs to axial skeleton
- Provide attachment for muscles
Clinicals:
- Fracture between medial 2/3 and lateral 1/3
- Lateral fragment pulled medial and forward by pectoralis major
- Injury to brachial plexus and axillary vessels
- Injury to subclavian artery
Sternum:

Sternal angle – angle formed by the junction of manubrium and body of sternum.
Importance: landmark to indicate level at which the 2nd rib joint with the sternum
Humerus:
- Medial epicondyle more outwards than lateral
- Lateral side – capitulum and deltoid tuberosity

Radius:
- Anterior surface smooth and concave at lower end
- Laterally – convex, lateral styloid process
- Medially – ulnar notch and medial tuberosity
- Lower end is large

Ulna:
- Medial styloid process
- Convex medially

Bones of hand:

From thumb to little finger:
- Trapezius, trapezoid, capitate, hamate
- Scaphoid, lunate, triquetral, pisiform
Muscle attachment on bones
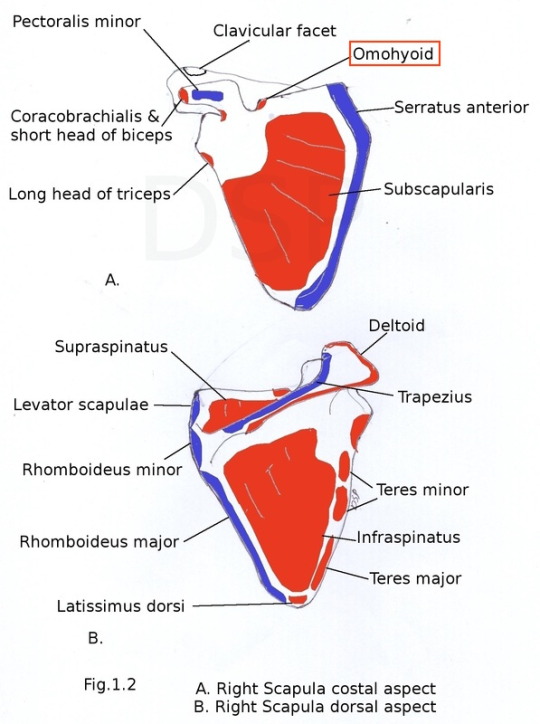





Clinicals:
- Dropped shoulder – trapezius paralyzed
- Winged shoulder – serratus anterior paralyzed
Arteries

NB: Same for deep veins of the arm, all deep veins are venae commitantes with the arteries.
(I) Axillary artery – chest, axilla, breast and shoulder joint
- Continuation of subclavian artery from lateral border of first rib
- Divided into 3 parts by passing posterior to pectoralis minor:
- 1st part – Superior thoracic
- 2nd part – Thoracoacromial and lateral thoracic
- 3rd part – Anterior circumflex humeral, posterior circumflex humeral, subscapular
- Continues as brachial artery from inferior border of teres major
(II) Brachial artery – all arm muscles and elbow joint
- Descends on ventral surface
- Medial to humerus
- Median nerve crosses over it from lateral to medial
- At apex of cubital fossa, divides into radial and ulnar arteries
- Other branches: profunda brachii (which gives middle and radial collateral), superior and inferior ulnar collateral and humeral nutrient artery
(III) Ulnar artery – anterior forearm muscles
- Descends obliquely on ulnar side and runs along ulnar border to wrist
- Deep to pronator teres
- Deep to superficial and intermediate muscles
- Lateral to ulnar nerve
- Superficial to flexor retinaculum
- Through Hook of Hamate and Guyon’s canal
- Divides into superficial and deep palmar arch
- Branches: anterior and posterior ulnar recurrent, common interosseous
(IV) Radial artery – posterior forearm muscles
- Descends obliquely on radial side and runs along radial border
- Anterior to pronator teres
- Winds around head of radius to go posterior
- Medial to radial nerve
- Through anatomical snuff box
- Divides into superficial and deep palmar arch
Veins
Superficial veins of arm:

NB: Cephalic V. used for:
- Drawing of blood
- Intravenous injection
- Venous cutdown
Nerves
Cutaneous innervation of upper limbs:


Dermatomes of upper limbs:



(I) Musculocutaneous nerve – anterior arm muscles, lateral forearm skin
- Roots – C5, C6, and C7
- At inferior border of pectoralis minor
- Pierce coracobrachialis muscle
- Runs between brachialis and biceps brachii
- Becomes lateral cutaneous nerve of forearm
- Runs in cubital fossa with cephalic vein
(II) Median nerve – anterior forearm muscles except flexor carpi ulnaris, elbow and wrist joint
- Roots – C5-T1
- The 2 cords join in axilla to form median nerve
- Crosses over brachial artery from lateral to medial
- Through cubital fossa
- Between 2 heads of pronator teres
- Through carpal tunnel
- Divides into recurrent and palmer digital nerves
Clinical: Carpal tunnel syndrome, hand of Benediction/ monkey hand
Entrapments: Carpal tunnel, cubital fossa, pronator teres heads
(III) Ulnar nerve – elbow joint, flexor carpi ulnaris and flexor digitorum profundus muscles
- Roots – C8-T1
- Runs in medial arm
- Passes posterior to medial epicondyle at elbow
- Between 2 heads of flexor carpi ulnaris
- Travels on the ulna side
- Superficial to flexor retinaculum
- Through hook of Hamate and Guyon’s canal
- Divides into superficial and deep branches
Clinical: Ulnar claw, fracture at medial epicondyl
Entrapments: Cubital tunnel, Guyon’s canal, flexor carpi ulnaris 2 heads
(IV) Radial nerve – Posterior arm and forearm muscles and skin
- Roots – C5-T1
- Posterior to axillary artery in axilla
- Posterior to brachial artery
- Between long and medial head triceps
- Exists via lower triangular space with profunda artery
- Runs in radial groove of humerus
- Pierce lateral intermuscular septum
- Anterior to lateral epicondyle of humerus
- Through cubital fossa
- Winds around neck of radius
- Penetrates supinator
- Descends between superficial and deep muscles of the posterior forearm
- Lateral to radial artery in anatomical snuff box
Clinicals:
- Injury in axilla/ humerus fracture – elbow, wrist and finger drop
- Injury in radial groove – wrist and finger drop
- Injury in radial head fracture – finger drop
- All have loss of sensation
Entrapments: Axilla, lower triangular space, radial groove, cubital fossa, anatomical snuff box

NB:
- Brachialis muscle supplied by both radial and musculocutaneous nerves
- Flexor digitorum profundus supplied by both ulnar and median nerves
(V) Axillary nerve – Glenohumeral joint, teres minor and deltoid muscle, skin of superolateral arm
- Roots – C5-C6
- Exists axilla via quadrangular space (with posterior circumflex humeral)
- Posterior division supplies teres minor
- Anterior division winds around neck of humerus – supplies anterior part of deltoid
Clinicals:
- Fracture of surgical neck
- Entrapment in quadrangular space
- Glenohumeral joint dislocation
- All this leads to paralysis of deltoid and teres minor and loss of skin sensation
Entrapments: Shoulder dislocations, axilla, quadrangular space
Joints
(I) Glenohumeral/shoulder joint
Classification: Ball and socket synovial
Articular surfaces: Head of humerus and glenoid fossa
Stability factors:
- Static: Coracoacromial arch (prevent superior displacement), coracoacromial ligament, glenohumeral ligament
- Dynamic: Rotator cuff muscles, deltoid, trapezius
Movements: Flexion, extention, abduction, adduction, medial and lateral rotation

NB: For abduction:
- 0 – 15 degrees – supraspinatus
- 15 -90 degrees – deltoid middle part
- 90 – 120 degrees – infraspinatus, teres minor
- 120 – 180 degrees – trapezius and serratus anterior
Blood supply: Anterior and posterior circumflex humeral
Nerve supply: Axillary, suprascapular
Clinicals: Due to shallow fossa, pulled anterior and inferior, damages axillary nerve
NB: Glenohumeral joint capsule has opening for biceps tendon
(II) Elbow joint
Classification: Synovial uniaxial hinge
Articular surfaces:
- Trochlea – trochlea notch on ulna
- Capitulum – head of radius
Stability factors:
- Static: Annular ligament, radial and ulnar collateral ligaments

2. Dynamic: Triceps, biceps, brachialis and radiobrachialis
Movements: Flexion and extension
Blood supply: Elbow anastomosis (written in arteries)
Nerve supply: Musculocutaneous, radial and ulna
Clinicals: Bursitis, dislocation, golfers elbow (medial epicondylitis), tennis elbow (lateral epicondylitis)
(III) Radioulnar joint
Proximal:
Classification: Synovial pivot uniaxial
Articular surfaces: Head of radius, radial notch on ulna
Stability factors: Annular ligament
Movements: Supination and pronation
Nerve supply: Musculocutaneous, median, radial and ulna
Distal:
Classification: Synovial pivot uniaxial
Articular surfaces: Ulna head and ulnar notch on radius
Movements: Supination and pronation
Blood supply: Anterior and posterior interosseous
Nerve supply: Anterior and posterior interosseous
Clinicals: Subluxation of radial head
(IV) Wrist joint
Classification: Ellipsoid synovial
Articular surfaces: Scaphoid, lunate, articular disc and distal end of radius
Stability factors:
1. Static: Joint capsule and ligaments:
- Palmer radiocarpal
- Dorsal radiocarpal
- Ulnar collateral – styloid process to trapezoid and pisiform
- Radial collateral – styloid process to scaphoid and trapezius
2. Dynamic: Carpal tunnel contents

Movements: Flexion, extension, abduction and adduction
Blood supply: Dorsal and palmer carpal arches
Nerve supply: Median nerve
Clinicals: Anterior lunate dislocation, carpal tunnel syndrome
(V) Sternoclavicular joint
Classification: Synovial saddle
Articular surfaces: Clavicle sternal end, manubrium of sternum, 1st costal cartilage
NB: Covered in fibrocartilage, separated into 2 compartments by articular disc
Stability factors: Anterior and posterior sternoclavicular ligament, interclavicular ligament, costoclavicular ligament

Clinicals: Anterior and posterior dislocations
(VI) Acromioclavicular joint
Classification: Plane synovial
Articular surfaces: Lateral end clavicle and acromion
NB: Covered in fibrocartilage, separated into 2 compartments by articular disc
Stability factors: Acromioclavicular ligament
Movements: Anterior and posterior
Clinicals: Suspend weight from upper limb from clavicle, dislocation

Others
1. Intervertebral disc – hyalin cartilage, shock absorber, hold adjacent vertebra together, distributes weight transmission
Clinicals: prolapsed IVD, herniation of IVD

2. Primary curvature – Kyphosis – thoracic and sacral
Secondary curvature – Lordosis – Cervical and lumbar

Clinical: Scoliosis

3. Mammary glands:
Extent:
Medially Laterally
2nd rib
Sternum ———-Mid axillary line
6th rib
- Axillary tail extends into axilla laterally
- Nipple at 4th intercostal space
Relations: overlies pectoral fascia covering 4 muscles
- Pectoralis major
- Serratus anterior
- External abdominis aponeurosis
- Rectus abdominis
Separated from fascia by retromammary space with loose connective tissue. This is the basis for free mobility of the breast chest wall
Base of breast ⇒ Retromammary space ⇒ Pectoral fascia
Blood supply:
- Perforationg branches of lateral thoracic
- Perforating branches of posterior intercostal arteries
- Superior thoracic
- Thoracoacromial
Nerve supply: 4th to 6th intercostal nerves
Lymphatic drainage:
- Internal mammary/ Internal thoracic
- Axillary (anterior, posterior, lateral and central)
- Supraclavicular nodes

Clinicals:
- Breast cancer – spread via lymphatics/venous channels. Due to axillary tail, axillary lymph nodes in breast cancer examined – swollen axillary nodes
- Mammography – radiography of breasts
- Masectomy – breast removal
- Mastities – infection through nipple during lactation
- Peau d’orange – ridges due to edema, inverted nipple
4. Triangle of auscultation – hear respiratory sounds
- Trapezius
- Scapular border
- Latissimus dorsi
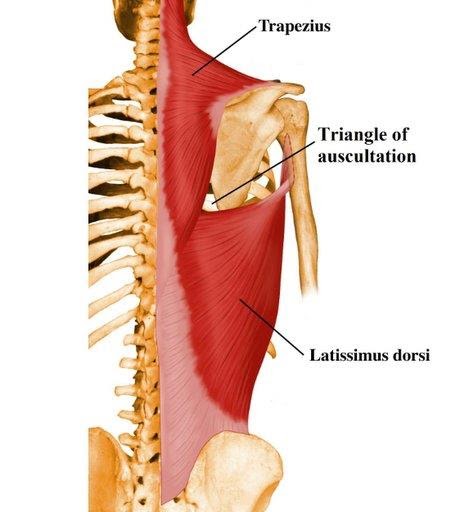
5. Deltopectoral triangle:

Contents: Cephalic vein and thoracoacromial branch
6. Clavipectoral fascia – fills gap between pectoralis minor and clavicle

7. Rotator cuff:
- Supraspinatus
- Infraspinatus
- Subscapularis
- Teres minor

Clinicals:
- Rotator cuff tendinitis (inflamed tendons)
- Rotator cuff tear (supraspinatus)
8. Spaces of the arm:

- Quadrangular space – Axillary nerve and posterior humeral circumflex vessels
- Upper triangular space – Circumflex scapular vessels
- Lower triangular space – Radial nerve and profunda brachii vessels
Clinicals: Entrapment syndrome
9. Axilla:

Boundaries:
- Anterior wall: Pec minor, pec major and clavipectoral fascia
- Medial wall: Serratus anterior, intercostal muscles, 1-4 ribs
- Lateral wall: Coracobrachialis, short head biceps brachii
- Posterior wall: Subscapularis, teres major, latissimus dorsi
- Base: Skin and fascia
- Apex:
- Anterior – clavicle
- Posterior – superior border scapula
- Medial – 1st rib
Contents:
- Axillary artery and vein
- Brachial plexus cords
- Axillary lymph nodes
- Axillary tail of breasts
Clinicals: Aneurysms, lymphomas
10. Cubital fossa:
Boundaries:

Contents: Medial to lateral
- Median nerve
- Brachial artery
- Biceps brachii tendon
- Radial nerve
Mnemonic: My Bottoms Turned Red
Clinicals:
- Brachial pulse
- Venepuncture – median cubital vein
- Cubital fossa syndrome
11. Carpal tunnel:
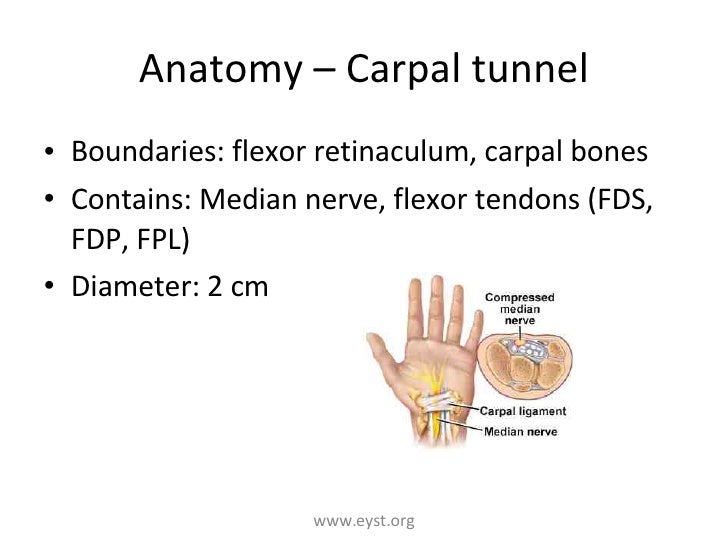
Anterior relations – Ulnar nerve and artery, palmaris longus tendon
Clinicals: Carpal tunnel syndrome – compressed median nerve, swollen tendons, thickened ligaments. Feelings of numbness and tingling
12. Anatomical snuff box:
Boundaries:
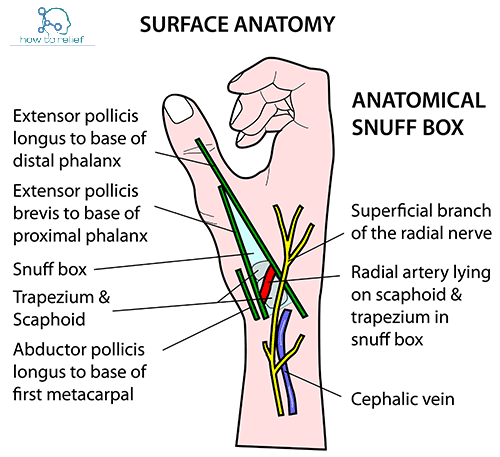
Floor – Scaphoid and trapezium
Contents:
- Radial artery
- Branch of radial nerve
- Cephalic vein
Clinical: Scaphoid fracture (arthritis, avascular, necrosis)
These are summarized notes from various sources, mainly TeachMeAnatomy and Wikipedia
