Stomach
Origin: Endodermal
- Lower part of foregut, swelling appears
- Anterior border connected to anterior abdominal wall by ventral mesogastrium
- Posterior border connected to posterior abdominal wall by dorsal mesogastrium
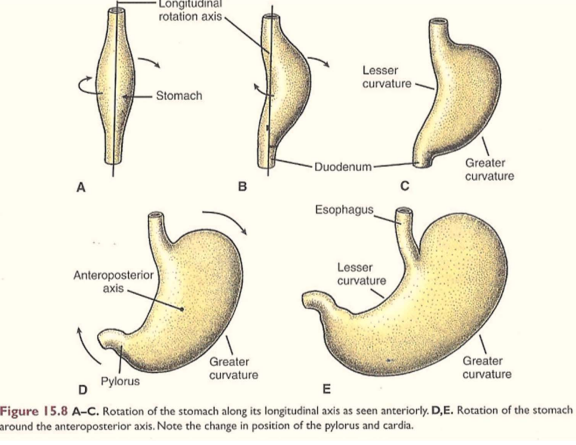
- Posterior border grows more – forms greater curvature of stomach
- Anterior border forms lesser curvature
- Stomach then rotates 90 degrees clockwise (due to growth of liver)
- So dorsal mesogastrium forms lesser sac
- Liver develops in ventral mesentery – mesentery becomes lesser omentum
- Spleen develops in dorsal mesentery – mesentery becomes gastrosplenic ligament
Clinicals: Congenital hypertrophy of pyloric sphincter – narrows pyloric canal. More common in males.
NB: Development of stomach and rotation causes right vagus nerve to become posterior vagus trunk. Left vagus nerve becomes anterior vagus trunk
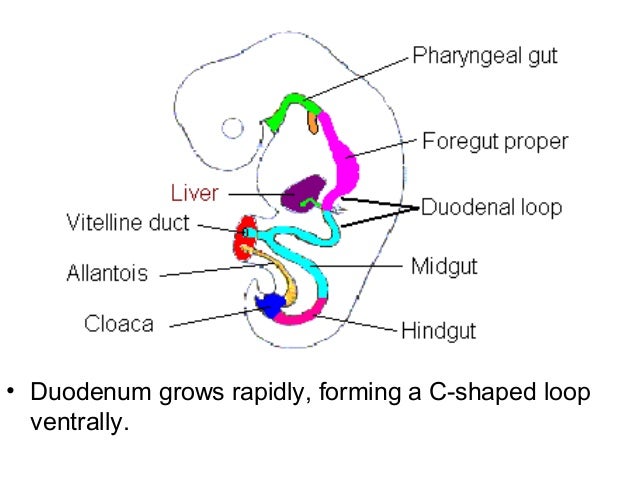
Duodenum
Origin: Endodermal
- Distal foregut and proximal midgut
- Form a “C” shaped loop projecting ventrally
- Due to stomachs rotation 90 degrees clockwise
- Duodenal loop carried dorsally and to the right, becomes adherent to posterior abdominal wall
- Mesentery of duodenum disappears except in the 1st and 4th part (ligament of trietz)
- The lumen is temporarily obstructed and canalized again
Congenital anomalies:
- Incomplete canalization/ atresia – green vomit, no bowel movement
- Incomplete fixation to posterior abdominal wall – sites of internal hernia
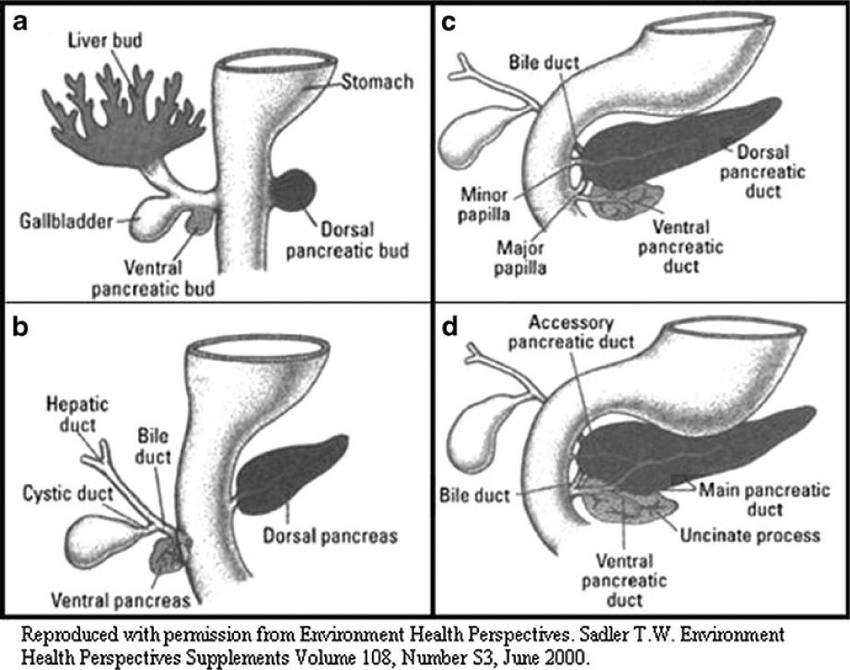
Pancreas
Origin: 2 endodermal buds form:
- Endoderm of dorsal wall of duodenum – dorsal pancreatic bud
- Endoderm of ventral wall of duodenum from hepatic bud stem – ventral pancreatic bud
- Dorsal pancreatic bud arises slightly above liver bud, extends dorsally and upwards into mesoduodenum
- Ventral pancreatic bud migrates dorsally to lie below and behind dorsal bud
- The 2 buds fuse together (ventral bud – head and uncinate process)
- Ducts of the 2 buds join – main pancreatic duct
- Islets of Langerhans appear – insulin secretion begins in 5th month
Congenital anomalies:
- Annular pancreas – develops as a ring around 2nd part duodenum
- Ectopic pancreatic tissue – eg. wall of duodenum, jejunum, ileum or stomach