Development of palatine tonsils, tongue and thyroid gland
Palatine tonsils
Origin: 2nd pharyngeal arch endoderm
Endoderm proliferates into buds ⇒ Canalizes ⇒ Forms crypts ⇒ Invaded by lymphocytes

Tongue
- Muscles of tongue – 3 occipital myotomes of paraxial mesoderm
- (1st occipital myotome forms extraoccular muscles of eye)
- The 3 remaining myotomes drag the hypoglossal nerve with them
2. Mucous membrane:
- Anterior 2/3 – 1st pharyngeal arch
- From two lingual swellings and tuberculum impar
- Posterior 1/3 – endoderm of 3rd pharyngeal arch
- Endoderm of 2,3 and 4 arch fuse to form Hypobronchial eminence
- A groove divides the hypobronchial eminence into:
- Upper part – Posterior 1/3 tongue mucous membrane
- Lower part – Forms epiglottis
Anterior and Posterior fuse at sulcus terminalis ( v shape)

Congenital anomalies:
- Aglossia – absence of tongue
- Macroglossia, microglossia
- Bifid tongue
- Glossoschisis – cleft tongue
- Tongue tie (ankyloglossia) – frenulum is till tip of tongue, can’t protrude tongue
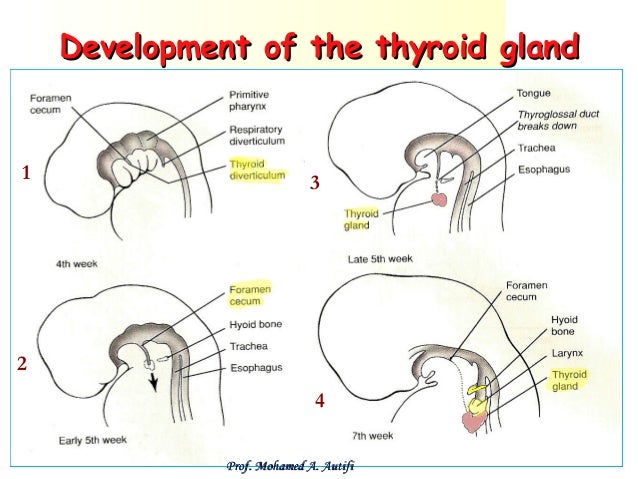
Thyroid gland
- Endodermal thickening around foramen cecum
- Forms thyroid primodium between tuberculum impar and hypobronchial eminance
- Thyroid primodium invaginated – bilobed diverticulum
- Descends infront of hyoid bone and laryngeal cartilage
- Connected to dorsum of tongue by thyroglossal duct
- Finally reaches infront of thyroid cartilage and upper trachea
- Thyroglossal duct obliterated
Congenital anomalies:
- Thyroid agenesis – absence, leads to stunted physical and mental growth
- Lingual thyroid – Fails to descend
- Thyroglossal cyst – thyroglossal duct unobliterated
- Thyroglossal fistula – cyst may rupture
- Ectopic positions – Sublingual, retrohyoid, retrosternal etc.
