Benign:
Primary malignancies of bone:

In patients own words, what is the problem
Previous treatments concerning the presenting complaint
Prenatal:
Natal:
Postnatal:
Vital signs:
NB: Also measure weight and height for children – to calculate BMI and dosage of LA and drugs
Remember it as: J A C C L O W D (Jaundice, anemia, clubbing, cyanosis, lymphadenopathy, oedema, wasting, dehydration)
Soft tissue examination:
Hard tissue examination:
Gingiva:
Oral hygiene:
Gingival index by Loe and Silness 1963:
Periodontal index by Turesky et al modified Quigley Hein 1970:
Index teeth and disclosing tablet
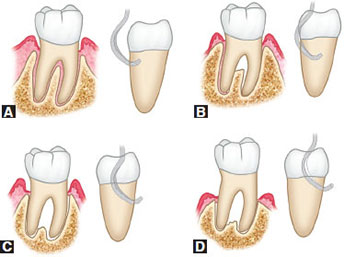
Furcation involvement – Glickman classification 1953
Periodontal charting:
1. Excellent prognosis:
2. Good prognosis:
3. Fair prognosis:
4. Poor prognosis:
5. Questionable prognosis:
6. Hopeless prognosis:
NB: Factors affecting prognosis:
General examination
Extraoral examination:
Intraoral examination:
Orthodontic examination:
OPG:
Study model analysis: Note date of impression, patient name, D.O.B, file number
a) Interarch analysis:
b) Intra arch analysis: Maxillary and mandibular
c) Space analysis:
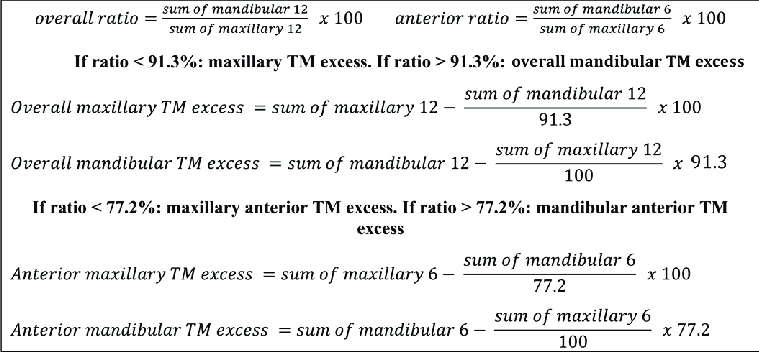
d) Bolton’s analysis: Maxillary and mandibular relationship for overbite/overjet
Sum of mandibular 12/Sum of maxillary 12 X 100 = 91.3% ± 1.91 (ie. range: 89.39-93.21)
e) Anterior ratio: Maxillary and mandibular relationship for overbite/overjet
Sum of mandibular 6/Sum of maxillary 6 X 100 = 77.2% ± 1.65 (ie. range: 75.55-78.85)
NB: Bolton’s analysis and anterior ratio cannot work if required teeth are missing
Photographs: Smile and profile analysis, record keeping
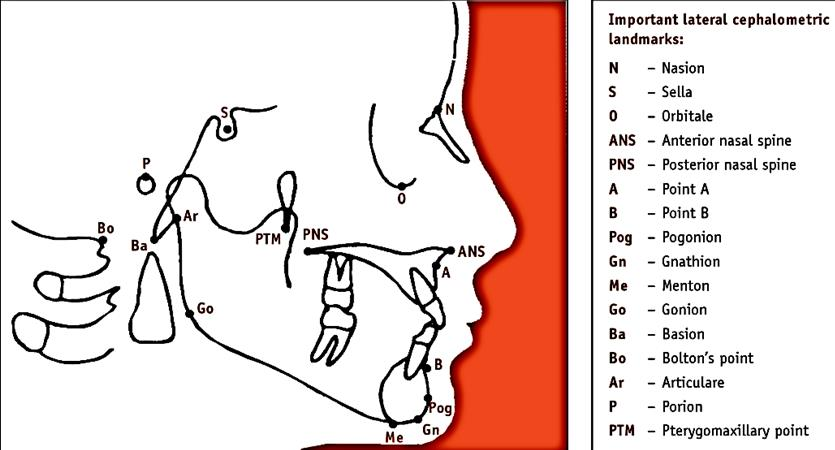
Lateral cephalogram analysis
Mixed dentition analysis using study models:
a) Radiograph/Huckaba analysis:
True width of 1st molar/Apparent width of 1st molar = True width of unerupted PM/Apparent width of unerupted PM
b) Moyer’s prediction table:

c) Tanaka and Johnston:
d) Nance – Arch perimeter analysis:
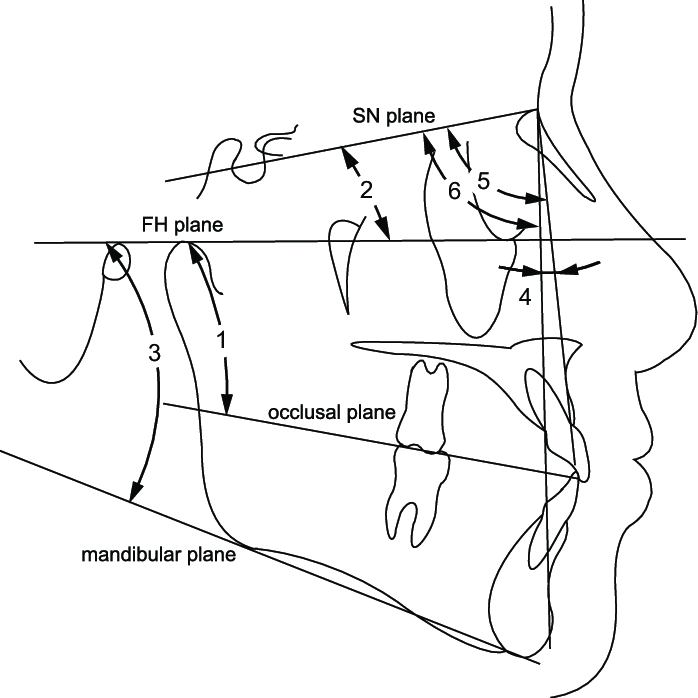
Skeletal analysis:
1. SNA angle: 82° ± 2
2. SNB angle: 80° ± 2
3. Angle ANB: 3 ± 1
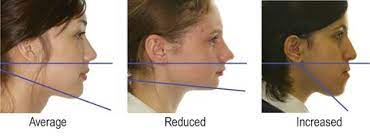
4. Mandibular plane angle: 32° ± 4
5. Occlusal plane angle: 17° ± 4
Dental analysis:
1. UI – NA angle and distance: 22°, 4mm
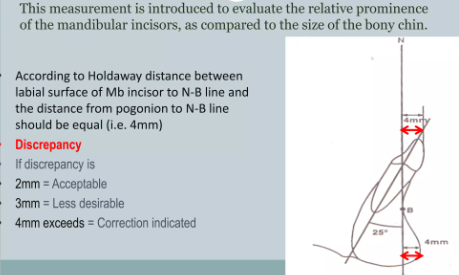
2. LI – NB angle and distance: 25°, 4mm
3. Interincisal angle: 130°-131°
4. Lower incisor to chin (Holdaway ratio)
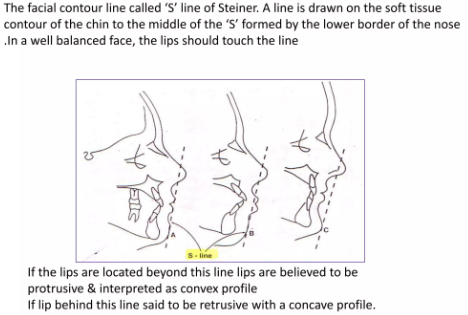
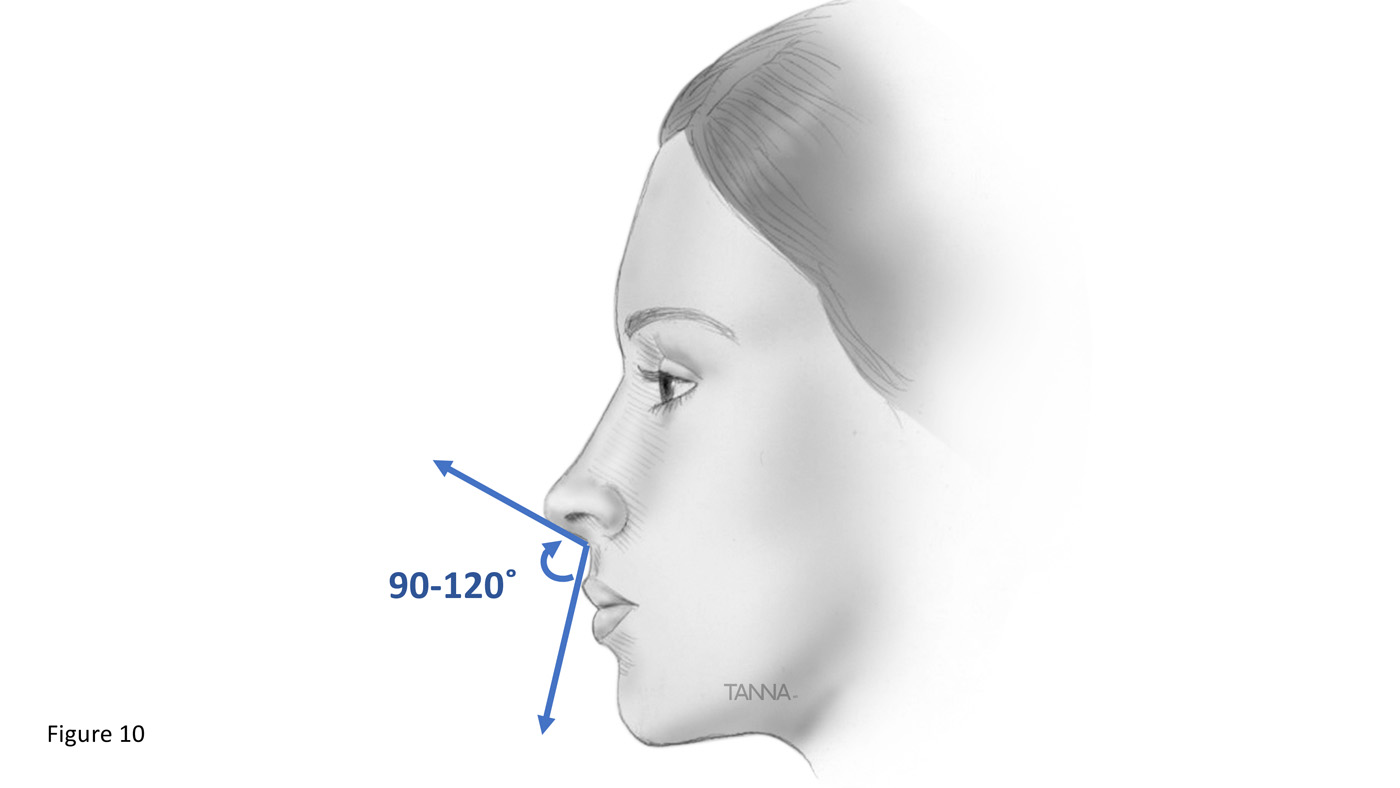
Soft tissue analysis:
Formerly known as histiocytosis x (eosinophilic granuloma, hand-schuller-christian disease, letterer-siwe disease)
Clinical: Short stature, diabetes insipidus, neurosensory deafness and tooth mobility
Radiology: Osteolysis causing ’floating teeth’ in multiple quadrants
Histology:
Management: Curettage of accessible bone lesions
Physiology: Vit C is required for redox reactions:
Clinical: Scurvy
Histology: Hemorrhagic gingival enlargement with minimal fibrosis
Management: Replacement therapy

Deficiency of vitamin D during bone development (infancy)
Etiology:
Physiology:
Clinical:
Histology: ↑ Osteoid matrix in bones
Lab:
Management: Replacement therapy
Etiology/classification:
1. Primary – Osteopenia without an underlying disease or medication
Contributing factors:
2. Secondary – due to:
A. Endrocrine disorders:
B. Neoplasia: multiple myeloma, carcinomatosis
C. Git problems: malnutrition, malabsorption, hepatic insufficiency, vit c & d deficiency
D. Medication: corticosteroids, anticonvulsants, heparin, alcohol
E. Miscellaneous: immobilization, anemias, pulmonary disease
Radiology: Enlargement of the medullary cavity + thinning of cortex
Histology:
Lab: ↑ serum phosphatase
Management: Hormone replacement therapy, manage other underlying causes
Abnormal and anarchic resorption and deposition, resulting in distortion and weakening of the affected bones
Epidemiology: M > F, patients over 50 years, Max > Mand (2:1)
Etiology:
Pathology:
Clinical:
Complication: (0.9 – 13%): progression to osteosarcoma
Histology:
X-ray:
Lab:
Management: Seldom fatal
Etiology: AD or sporadic form – osseous growth spurt during development.
Common sites:
Radiology: Mandibular enlargement, cortical redundancy
Lab:
Management: Symptomatic
Etiology:
Clinical:
Management: Gradual replacement therapy + synthetic and natural thyroid hormone preparations.