Tell – Explain procedure with age appropriate language
Show – Demonstrate procedure
Do – Perform procedure
Communication should be gentle, addressing the child. Use euphemism (eg. call LA “sleeping juice”, rubber dam “umbrella”) and smile. Have positive reinforcement.
2. Behavior modelling – Show other children getting procedures and how they behave
3. Distraction – Music, videos, virtual reality
4. Relaxation therapy – Relaxation exercises to do at home
5. Systemic desensitization – Present the procedure in a graduated fashion to reduce anxiety
6. Hypnosis – Altered state of consciousness to produce desirable behavior
7. Aversive techniques: Must obtain parent consent, informed consent, document indication and duration. Should be legal in country of practice and be used with extreme caution.
Hand over mouth – and explain in child’s ear. Contraindicated in children below 3 and special health care needs
Protective stabilization – can cause physical and psychological harm. Active is by dental team, passive is by protective devices
Voice control – Changing volume, speed or tone of voice to get child’s attention
Use the app Dental Drugs (App store, Play store) to quickly refer for prescribing medications, calculating maximum anesthetic dosages or recalling common treatment/emergency protocols in practice
Use the app Dental Drugs (App store, Play store) to quickly refer for prescribing medications, calculating maximum anesthetic dosages or recalling common treatment protocols in practice
Desirable properties of LA
Non irritant
Reversible effect
Long enough duration for procedure
Low toxicity
Fast onset of action
Potent
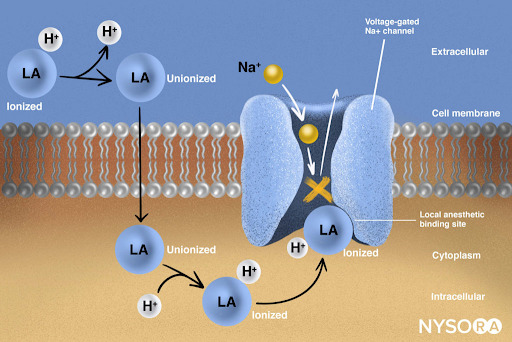
Mechanism of action of LA
LA = Tertiary amine base [B] + Water soluble hydrochloride [B.HCl]
Injected into tissues
Base liberated in alkaline pH of tissues
B.HCl + HCO3 = B + H2CO3 + Cl
Base diffuses through nerve sheath into axoplasm and partially ionizes
B + H+ = BH+
Ionized form of BH+ enters sodium channel from interior of nerve and combines with a specific receptor in the channel to block sodium influx into the nerve and therefore prevent action potential initiation
BH+ + Receptor = Block sodium influx
Structure of LA
Aromatic group – Intermediate bond (amide/esters)- Tertiary amine
Amides:
Lignocaine
Prilocaine – metabolism in liver and lungs. Primary product of metabolism is ortho-Toluidine – associated with methemoglobinemia
Mepivacaine
Bupivacaine
Esters:
Cocaine – Only cocaine causes vasoconstriction
Procaine – used in case of drug induced arteriospasm. Procaine broken down to PABA – associated with allergic reaction.
Amethocaine
Chloroprocaine
Factors affecting LA action
1. pKa (physiologic pH): ↓ pKa leads to faster onset of action as ↑ molecules diffuse through the nerve sheath
2. Lipid solubility: ↑ lipid solubility leads to ↑ potency and therefore block conductions at low concentration
3. Protein binding: ↑ protein binding leads to ↑ duration of action as it firmly attaches to proteins at receptor sites
4. Non nervous tissue diffusibility: ↑ diffusibility leads to slower time of onset
5. Vasodilator activity: ↑ vasodilator activity leads to ↑ blood flow to region and therefore ↑ removal of anesthetic molecules and so ↓ potency and duration
6. Tachyphylaxis: ↑ tolerance when injected repeatedly. Mop up of HCO3, alkaline pH of tissues not sustained
7. Infection: Acidic pH therefore prevent ready formation of free base
Contents of LA
Local anesthetic agent
Lignocaine HCL
Block nerve conduction
Vasoconstrictor
Epinephrine
– Increase duration by decreasing absorption of LA – Control bleeding – Prevent systemic toxicity
Pseudocholinesterase also metabolize succinylcholine – therefore atypical pseudocholinesterase associated with difficult general anesthesia (sleep apnea). Succinylcholine used to cause short term paralysis as part of GA
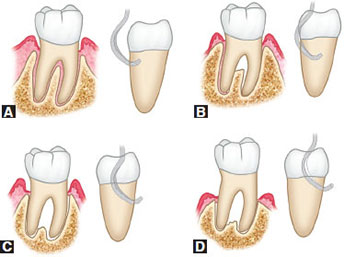
Grade 1 – Incipient, pocket formation into furcation fluting, interradicular bone intact
Grade 2 – Moderate loss of interradicular bone but not through and through
Grade 3 – Probe goes through and through, orifice occluded by gingival tissue
Grade 4 – Exposed furcation
Periodontal charting:
Draw continuous line of free gingival margin – facial and lingual
Draw interrupted line indicating bone level on facial side
Record 6 point pocket depth
Record tooth mobility
Record missing teeth (X), open contacts(//) and how many mm, overhang restorations (V)
Calculate clinical attachment loss (CAL): Gingival recession + pocket depth
1-2mm = Mild
3-4mm = Moderate
> 5mm = Severe
Localized: < 30% of sites
Generalized: > 30% of sites
Orthodontic assessment
A-P: Molar, canine, incisor relationship – Class I, II, III
Vertical: Open bite, overbite – deep or open
Transverse:
Crossbite anterior or posterior
Midlines
Crowding or spacing
Rotation or displacement
Proclination
Upper and lower arch form – Normal, V shape, square shape
Investigations
Radiological – describing a x-ray:
Name and age of patient
Date when the x-ray was taken
Quality
Teeth present
Dental age and why
Radiolucent/radiopaque lesions
Microbiological
Histopathological
Study model
Diet chart
Plaque score
BMI
Diagnosis
Summarize findings: eg. A 5 year old African male with early childhood caries, dentoalveolar abscess secondary to extensive decay on 55, irreversible pulpitis 85 and 75, and occlusal caries on 54, 64, 84, 74
For periodontal diagnosis: Severity – extent – diagnosis, eg:
Mild – localized – chronic periodontitis
Moderate – generalized – plaque induced gingivitis secondary to orthodontic treatment and mouth breathing
Prognosis for periodontology
1. Excellent prognosis:
No bone loss
Excellent gingival condition
Good patient co-operation
No systemic/environmental factors
2. Good prognosis:
Adequate remaining bone support
Adequate control of etiologic factors and maintainable dentition
Adequate patient co-operation
No systemic/environmental factors or well controlled
3. Fair prognosis:
Less than adequate bone support
Some tooth mobility
Grade 1 furcation
Adequate maintenance possible
Acceptable patient co-operation
Presence of limited systemic/environmental factors
4. Poor prognosis:
Moderate-advanced bone loss
Tooth mobility
Grade 1 or 2 furcation involvement
Doubtful patient co-operation
Presence of systemic/environmental factors
5. Questionable prognosis:
Advanced bone loss
Tooth mobility
Grade 2 or 3 furcation involvement
Inaccessible areas
Systemic/environmental factors
6. Hopeless prognosis:
Advanced bone loss
Extraction indicated
Non maintainable areas
Uncontrolled systemic/environmental factors
NB: Factors affecting prognosis:
Diagnosis: Disease severity, plaque and calculus
Systemic factors: DM, puberty, genetic
Occlusal factors
Prosthetic and restorative factors: Caries, teeth vitality, abutment selection, subgingival restorations, fixed or removable prosthesis
Subdivision: if right or left unilateral Angles class II
Angles class III:
Type 1: Edge to edge bite
Type 2: Normal overbite
Type 3: Anterior cross bite
Pseudo class III malocclusion: Mandible moves forward
Vertical plane:
Overbite: Normal 20-40%. <20% = reduced overbite, >40% = deep bite
Open bite
Anterior crossbite/ reverse overjet
Transverse plane:
Midline
Crossbite
Scissor bite
Investigation
OPG, study model, photograph, lateral cephalogram, CT scan
OPG:
Name and age of patient
Date when the x-ray was taken
Quality
Teeth present
Dental age, development of crown and roots, root completion 2-3 years after eruption
Radiolucent/radiopaque lesions
Study model analysis: Note date of impression, patient name, D.O.B, file number
a) Interarch analysis:
A-P, transverse, vertical plane
Use dividers to measure
b) Intra arch analysis: Maxillary and mandibular
Shape (U, V)
Arch symmetry (position of teeth, missing teeth)
Palate vault
Number of teeth present, or eupting
Individual tooth malformation, malposition, or rotation
c) Space analysis:
Arch parameter (X) = Measure arch from 5 to 5, distal surface
Tooth material (Y)= Width of each tooth. Angles lines of occlusion:
Maxillary – use central fossa and cingulum (in anterior teeth)
Mandible – use buccal cusp tips and incisal edges
Difference between arch parameter and tooth material:
X – Y = Positive (spacing), Negative (crowding)
≤ 4mm = Mild crowding
5-8 mm = Moderate crowding
> 9mm = Severe crowding
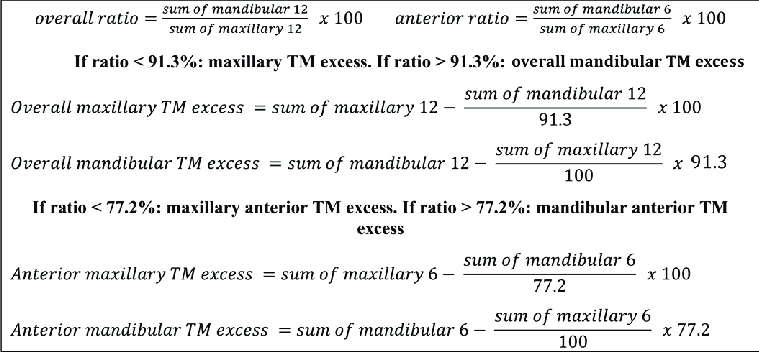
d) Bolton’s analysis: Maxillary and mandibular relationship for overbite/overjet
Sum of mesiodistal width of 12 teeth: CI, LI, C, PM, PM, M1 on both sides
Sum of mandibular 12/Sum of maxillary 12 X 100 = 91.3% ± 1.91 (ie. range: 89.39-93.21)
< 91.3% = Maxillary teeth in excess
>91.3% = Mandibular teeth in excess
e) Anterior ratio: Maxillary and mandibular relationship for overbite/overjet
Sum of mesiodistal width of 6 teeth: CI, LI, C on both sides
Sum of mandibular 6/Sum of maxillary 6 X 100 = 77.2% ± 1.65 (ie. range: 75.55-78.85)
< 77.2% = Anterior maxillary teeth in excess
>77.2% = Anterior mandibular teeth in excess
NB: Bolton’s analysis and anterior ratio cannot work if required teeth are missing
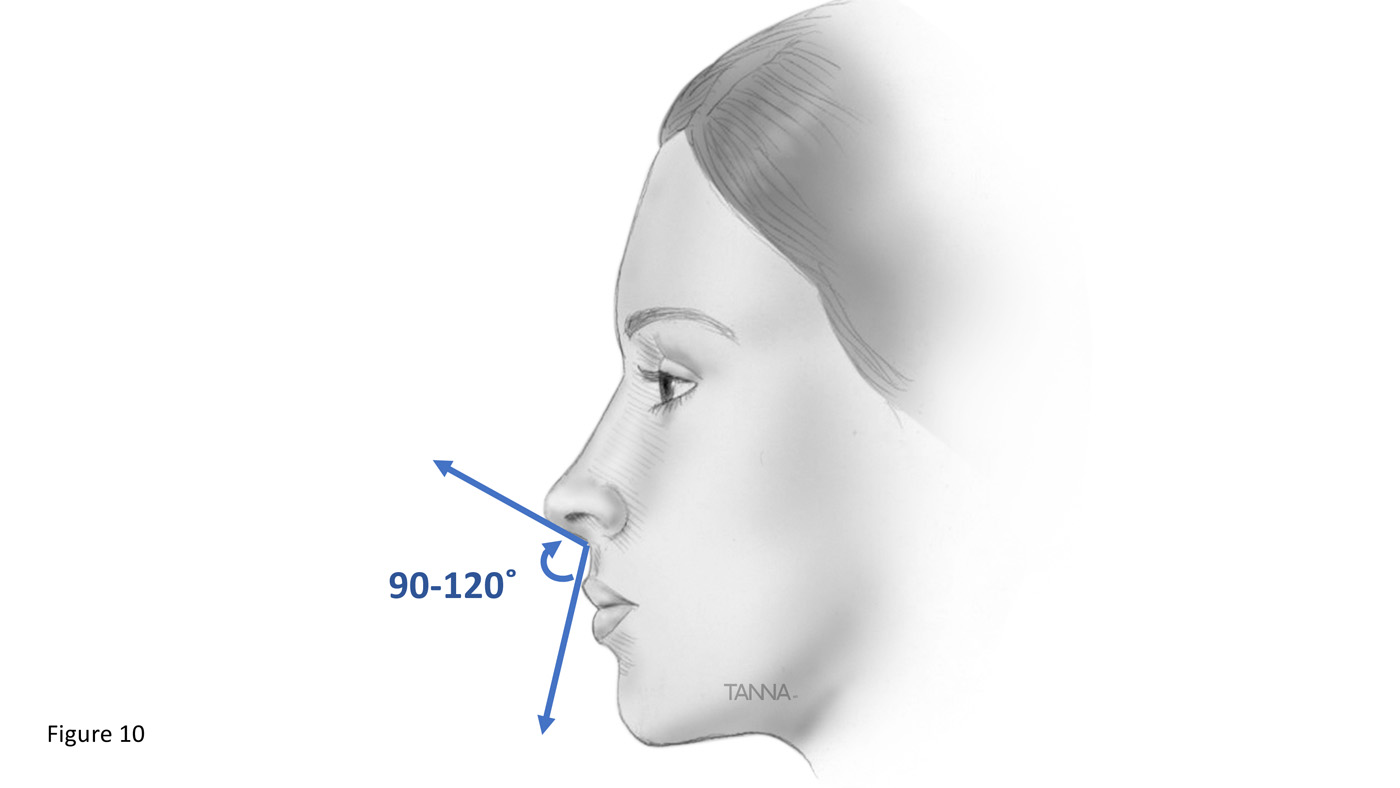
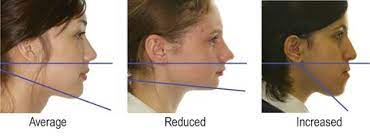
Photographs: Smile and profile analysis, record keeping
Lateral cephalogram analysis
Mixed dentition analysis using study models:
a) Radiograph/Huckaba analysis:
True width of 1st molar/Apparent width of 1st molar = True width of unerupted PM/Apparent width of unerupted PM
b) Moyer’s prediction table:
Use sum of mandibular 4 incisors to predict mesiodistal width of permanent canine and premolars
75 percentile usually used
c) Tanaka and Johnston:
Estimated mesiodistal width of canine and premolar of one quadrant = 1/2 of the mesiodistal width of mandibular 4 incisors + 10.5mm (for mandible) or 11mm (for maxilla)
d) Nance – Arch perimeter analysis:
Mesiodistal width of erupted permanent teeth and from IOPA of unerupted teeth
Diagnosis
List name, age and gender
Write problem list in priority
Eg. Angles class I malocclusion with an anterior open bite extending from 15/45 to 25/35, with an overjet of 6mm and tongue thrusting habit
Treatment plan
List treatment objectives according to PC and priority
List treatment plan
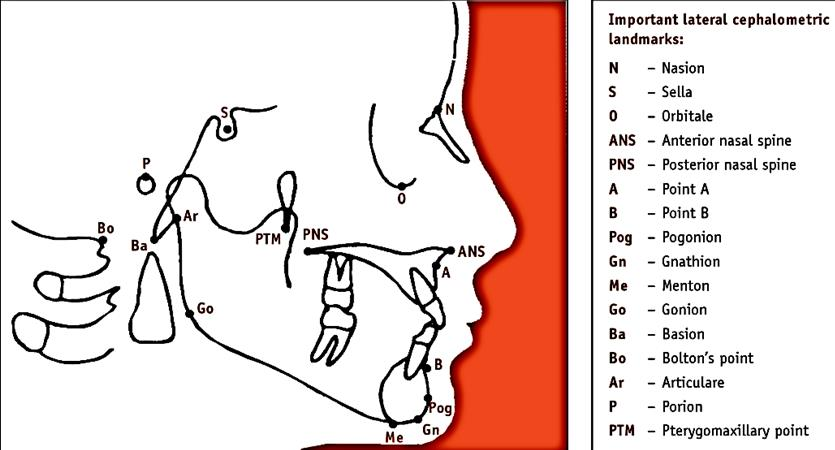
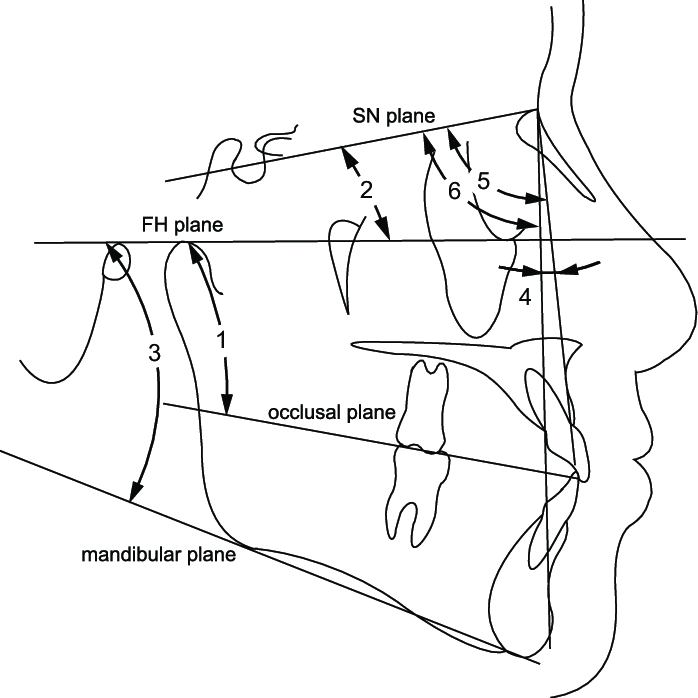
Cephalometric analysis
S – Sella turcica – center of pituitary fossa
N – Most anterior point of frontal and nasal bone junction
A – Inner most point between ANS and incisor
B – Inner most point between mandible and incisor
Pog – Anterior most point of mandible
Gn – Most anterior inferior point of bony chin
Go – Point where posterior border of ramus and lower border of mandible bisect