History:
- Biodata
- Presenting complain
- HPC
- PDH
- Dental habits
- PMH
- FSH
- Birth history
- Abnormal habits
Clinical examination:
General examination
Extraoral examination:
- JACCLOWD
- TMJ movements – clicking or popping sounds, pain, path of closure
- Facial profile
- Facial symmetry
- Lip competency
- Incisor showing on smiling – Normally 2-4mm
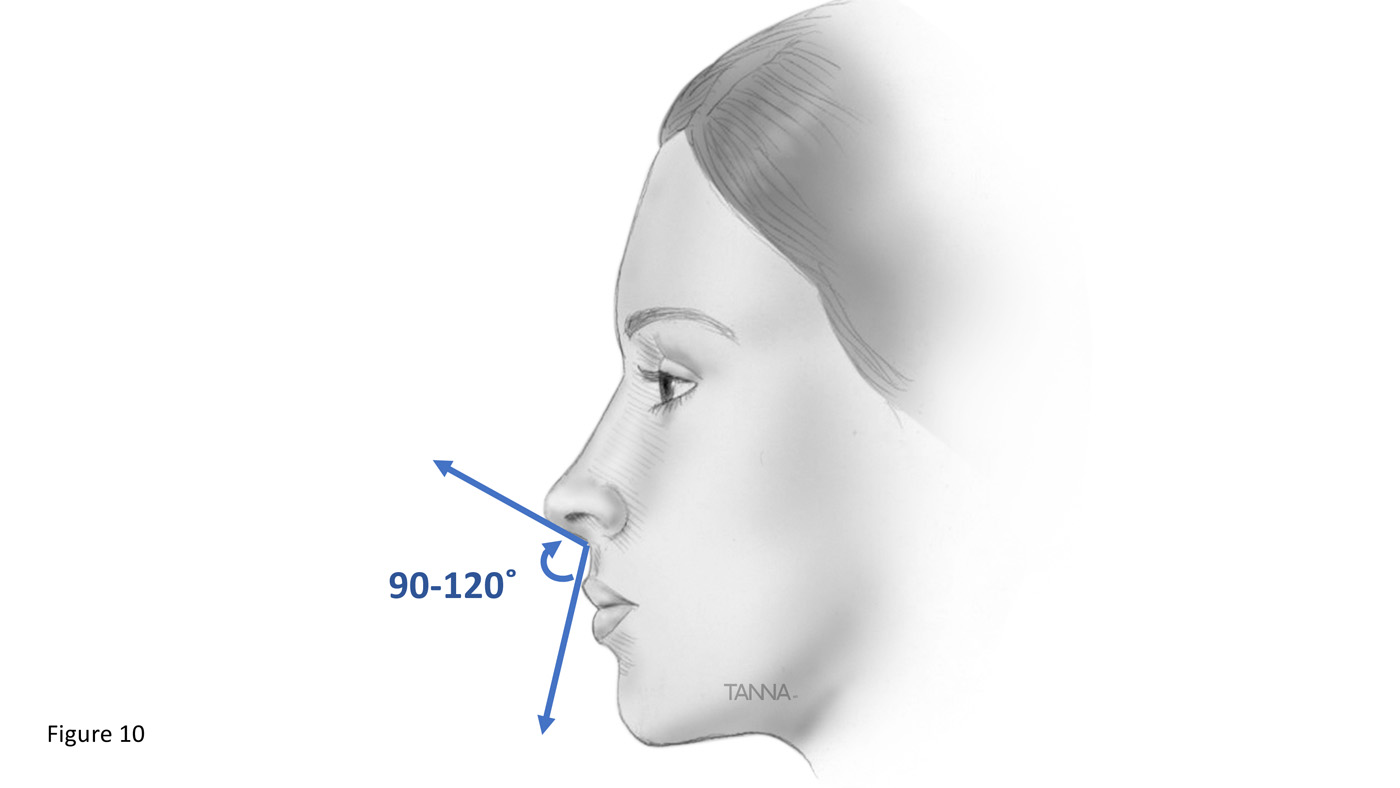
- Nasolabial angle and lip protrusion:
- Between upper lip and base of nose
- Normal 90° – 110°
- Convex – Class II, retrusive mandible
- Concave – Class III, protrusive mandible
- Becomes retrusive and obtuse angle with age
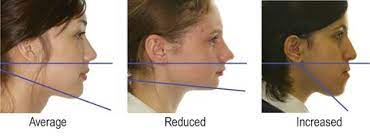
- Vertical facial relationship – Angle of lower border of mandible to cranium
- Use occipital region to draw imaginary line
- Average
- Reduced – Short face syndrome: Deep bite, overlapped lips
- Increased – Long face syndrome: Anterior open bite, incompetent lips
Intraoral examination:
- Oral hygiene status
- Type of dentition: primary, mixed, permanent
- Soft tissue and hard tissue examination
- Dental arches:
- Crowding: mild, moderate, severe
- Spacing
- Tooth rotations: mesioversion, distoversion lingoversion, buccoversion, labioversion)
- Tooth displacement
- Ugly duckling stage
Orthodontic examination:
- Anterior – posterior plane: Molar, canine, incisor relationship – Class I, II, III
- Molar malocclusions: Maxillary 6 MB cusp and mandibular 6 buccal groove.
- Angles class I: 7 types:
- 1. Maxillary teeth crowded
- 2. Anterior teeth proclined
- 3. Anterior crossbite
- 4. Posterior crossbite
- 5. Permanent molars drifted mesially
- 6. Diastema
- 7. Deep overbite
- Angles class II:
- Division I: Incisors proclined
- Division II: Incisors retroclined
- Subdivision: if right or left unilateral Angles class II
- Angles class III:
- Type 1: Edge to edge bite
- Type 2: Normal overbite
- Type 3: Anterior cross bite
- Pseudo class III malocclusion: Mandible moves forward
- Angles class I: 7 types:
- Molar malocclusions: Maxillary 6 MB cusp and mandibular 6 buccal groove.
- Vertical plane:
- Overbite: Normal 20-40%. <20% = reduced overbite, >40% = deep bite
- Open bite
- Anterior crossbite/ reverse overjet
- Transverse plane:
- Midline
- Crossbite
- Scissor bite
Investigation
- OPG, study model, photograph, lateral cephalogram, CT scan
OPG:
- Name and age of patient
- Date when the x-ray was taken
- Quality
- Teeth present
- Dental age, development of crown and roots, root completion 2-3 years after eruption
- Radiolucent/radiopaque lesions
Study model analysis: Note date of impression, patient name, D.O.B, file number
a) Interarch analysis:
- A-P, transverse, vertical plane
- Use dividers to measure
b) Intra arch analysis: Maxillary and mandibular
- Shape (U, V)
- Arch symmetry (position of teeth, missing teeth)
- Palate vault
- Number of teeth present, or eupting
- Individual tooth malformation, malposition, or rotation
c) Space analysis:
- Arch parameter (X) = Measure arch from 5 to 5, distal surface
- Tooth material (Y)= Width of each tooth. Angles lines of occlusion:
- Maxillary – use central fossa and cingulum (in anterior teeth)
- Mandible – use buccal cusp tips and incisal edges
- Difference between arch parameter and tooth material:
- X – Y = Positive (spacing), Negative (crowding)
- ≤ 4mm = Mild crowding
- 5-8 mm = Moderate crowding
- > 9mm = Severe crowding
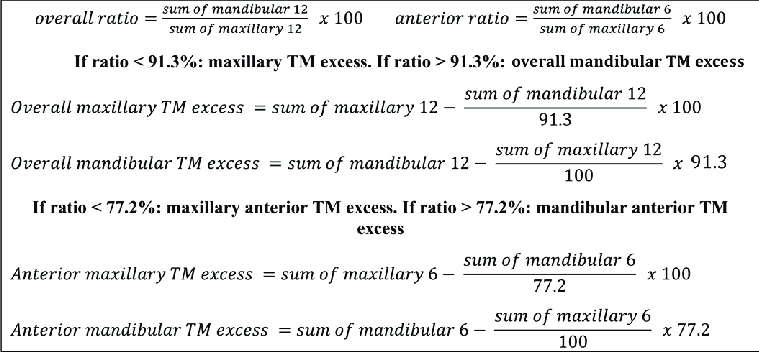
d) Bolton’s analysis: Maxillary and mandibular relationship for overbite/overjet
- Sum of mesiodistal width of 12 teeth: CI, LI, C, PM, PM, M1 on both sides
Sum of mandibular 12/Sum of maxillary 12 X 100 = 91.3% ± 1.91 (ie. range: 89.39-93.21)
- < 91.3% = Maxillary teeth in excess
- >91.3% = Mandibular teeth in excess
e) Anterior ratio: Maxillary and mandibular relationship for overbite/overjet
- Sum of mesiodistal width of 6 teeth: CI, LI, C on both sides
Sum of mandibular 6/Sum of maxillary 6 X 100 = 77.2% ± 1.65 (ie. range: 75.55-78.85)
- < 77.2% = Anterior maxillary teeth in excess
- >77.2% = Anterior mandibular teeth in excess
NB: Bolton’s analysis and anterior ratio cannot work if required teeth are missing
Photographs: Smile and profile analysis, record keeping
Lateral cephalogram analysis
Mixed dentition analysis using study models:
a) Radiograph/Huckaba analysis:
True width of 1st molar/Apparent width of 1st molar = True width of unerupted PM/Apparent width of unerupted PM
b) Moyer’s prediction table:
- Use sum of mandibular 4 incisors to predict mesiodistal width of permanent canine and premolars
- 75 percentile usually used

c) Tanaka and Johnston:
- Estimated mesiodistal width of canine and premolar of one quadrant = 1/2 of the mesiodistal width of mandibular 4 incisors + 10.5mm (for mandible) or 11mm (for maxilla)
d) Nance – Arch perimeter analysis:
- Mesiodistal width of erupted permanent teeth and from IOPA of unerupted teeth
Diagnosis
- List name, age and gender
- Write problem list in priority
- Eg. Angles class I malocclusion with an anterior open bite extending from 15/45 to 25/35, with an overjet of 6mm and tongue thrusting habit
Treatment plan
- List treatment objectives according to PC and priority
- List treatment plan
Cephalometric analysis
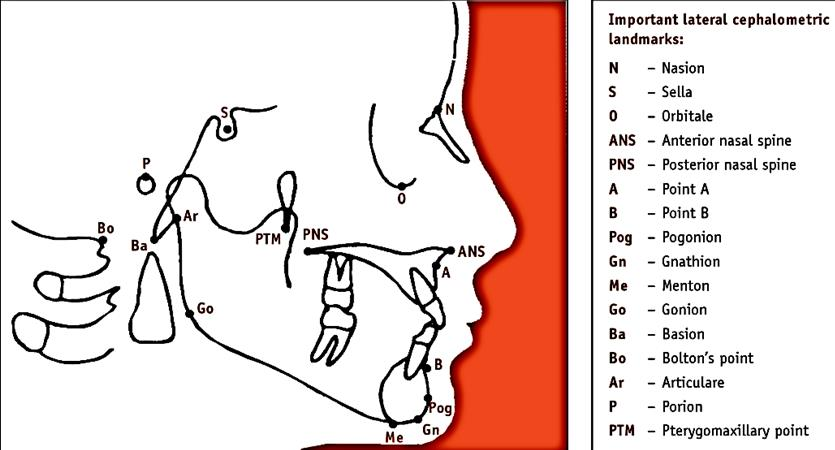
- S – Sella turcica – center of pituitary fossa
- N – Most anterior point of frontal and nasal bone junction
- A – Inner most point between ANS and incisor
- B – Inner most point between mandible and incisor
- Pog – Anterior most point of mandible
- Gn – Most anterior inferior point of bony chin
- Go – Point where posterior border of ramus and lower border of mandible bisect
- Porion – External auditory meatus upper contour midpoint
- Orbitale – Inferior margin of orbit – lowest point
- Frankfort plane (FH) – Porion to orbitale
- Occlusal plane – Use molars and premolars
- Mandibular plane – Gn to Go
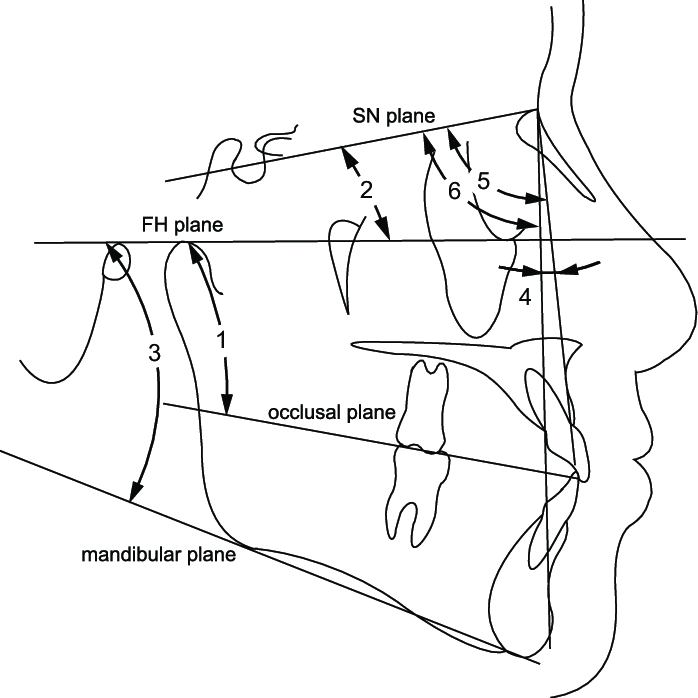
Steiner’s analysis
Skeletal analysis:
1. SNA angle: 82° ± 2
- Ant-post position of maxilla with cranial base
- Increased angle = Prognathic maxilla
2. SNB angle: 80° ± 2
- Ant-post position of mandible with cranial base
3. Angle ANB: 3 ± 1
- Difference between SNA and SNB – magnitude of skeletal jaw discrepancy
- Factors affecting:
- Vertical height of face
- Abnormal position of nasion
- Increased angle = Class II
- Decreased angle = Class III
4. Mandibular plane angle: 32° ± 4
- Steepness of mandibular plane to cranial base
- Increased angle = Vertical growth
- Decreased angle = Horizontal growth
5. Occlusal plane angle: 17° ± 4
- Determine relationship of teeth in occlusion with cranial base
- Increased angle = Skeletal open bite
- Decreased angle = Skeletal deep bite
Dental analysis:
1. UI – NA angle and distance: 22°, 4mm
- > 4mm or increased angle = Protrusion eg. class II division 1
- < 4mm or decreased angle = Retrusion eg. class II division 2
2. LI – NB angle and distance: 25°, 4mm
- > 4mm or increased angle = Protrusion eg. class II division 1
- < 4mm or decreased angle = Retrusion eg. class II division 2/ class III
3. Interincisal angle: 130°-131°
- Increased angle = Class II division 2
- Decreased angle = Class II division 1
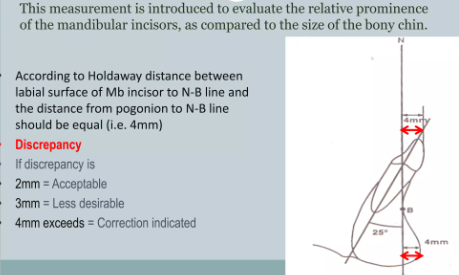
4. Lower incisor to chin (Holdaway ratio)
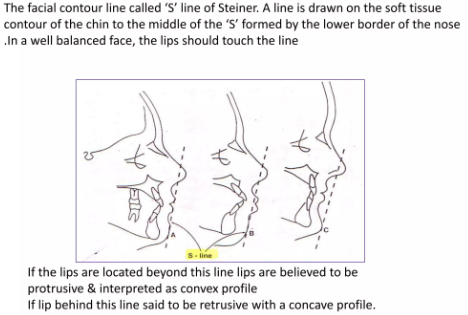
Soft tissue analysis:

2 thoughts on “Orthodontic History, Examination, Investigation, Treatment Planning and Cephalometric Analysis”
Comments are closed.