History
Biodata
- Date
- File number
- Full name
- Age/date of birth
- Gender
- Contact
- Physical address
- Occupation
- Name of guardian/parent – for children
- Source of referral (if referred)
Presenting complaint
In patients own words, what is the problem
History of presenting complaint
- S – Site
- O – Onset
- C – Character (throbbing, continuous, dull, acute, sharp)
- R – Radiation (to head)
- A – Associated symptoms (fever, discharge)
- T – Timing (day or night, after eating)
- E – Exacerbating factors (hot/cold food), Alleviating factors (Pain medications)
- S – Scale (scale of 1-10, rate the pain)
Previous treatments concerning the presenting complaint
Past dental history
- Index visit or
- Previous dental treatments done
- What they were
- When
- Where
- If extraction done – any complications
- Tolerance to LA
Dental habits
- How many times do they brush their teeth
- How do they brush
- Which toothpaste
- How often they change their brush
- Any interdental cleaning methods used – floss, toothpicks
- Abnormal habits eg. mouth breathing, lip sucking
Past medical history
- History of chronic illness:
- CHD/CVS, infective endocarditis
- Respiratory – asthma, bronchitis
- GIT – peptic ulcers, diarrhea, vomiting, jaundice, hepatitis, gastritis
- Diabetes
- CNS disorders
- Bleeding disorders – hemophilia, anticoagulant therapy
- Infectious diseases – TB, HIV, Herpes
- On any medications – NSAID, corticosteroids, anticoagulants, anticonvulsants
- Previous hospital admission – When, where, why, treatment provided
- Food or drug allergy
Obs and gyn history for females
- Last menstruation date and regularity
- Pregnancy status
- Type of contraceptives used
Family social history
- Alcohol – amount and frequency
- Smoking – amount and frequency
- Drugs
- Family status – parents, siblings, chronic illness in family
- Martial status and children
- Water source – borehole or city council
For pediatric and orthopedic patients
Birth history:
Prenatal:
- Health and nutritional status of mother during pregnancy
- Complications during pregnancy:
- Infections – rubella, TB, syphilis, UTI
- Pre-eclampsia
- Hypertension
- Diabetes
- Antepartum bleeding
- Drugs
- X-ray
- Rh incompatibility may result in erythroblastosis fetalis – leading to green blue discoloration of dentition. Picture
Natal:
- Full term or premature
- Mode of delivery – Normal/C-section and why?
- Did the baby cry on birth
- Birth weight
- Breast fed or formula milk given
Postnatal:
- Vaccinated
- Developmental history
- Nocturnal feedings/sweetened milk – predisposes to early childhood caries (read more)
- Brushing habits – frequency, by who, supervised?
Habits
- Finger sucking/thumb sucking
- tongue thrusting
- Mouth breathing
- Nail biting – check nails
Diet chart
- 24 hour diet chart
- 7 day diet chart (as investigation)
Family social history
- Name of school
- Class
- Performance in school
- Social or antisocial
- Occupation of parents
- Family history
- Water source
Clinical examination
General examination
- Anxious or calm
- Build, nourishment – well, poor
- Posture
Vital signs:
- Temperature
- Pulse rate
- Respiratory rate
- Blood pressure
NB: Also measure weight and height for children – to calculate BMI and dosage of LA and drugs
Extra oral examination
- Palpate submental, submandibular and neck lymph nodes
- Facial symmetry – any swellings or asymmetry
- Facial profile
- Scars
- Eyes – jaundice (look down), pallor (look up)
- TMJ movements – clicking or popping sounds, pain, path of closure
- Lips competency
- Hands – examine nails, finger clubbing, cyanosis
Remember it as: J A C C L O W D (Jaundice, anemia, clubbing, cyanosis, lymphadenopathy, oedema, wasting, dehydration)
Intraoral examination
- Oral hygiene status
- Type of dentition: primary, mixed, permanent
Soft tissue examination:
- Gingiva – shape, size, color, bleeding, ulceration, growths, pockets, recession
- Plaque and gingival score
- Buccal mucosa – color, texture, ulcer, growth, sinus
- Floor of mouth – swellings, ulcer
- Tongue – size, movements, plaque
- Palate – normal, high vault, clefts
- Tonsils – normal, swollen
- Frenal attachments – normal, higher
Hard tissue examination:
- According to quadrants
- Teeth present
- Teeth missing
- DMF
- Palpate, percuss
- Check interproximal caries with floss
- Wear (attrition, abrasion, erosion)
- Discoloration
- Malformation
- Mobility – Millers classification 1950
- 0 = No detectable mobility
- 1 = Distinguishable mobility
- 2 = Horizontal movement > 1mm
- 3 = Horizontal and vertical movement > 1mm
- Orthodontic assessment
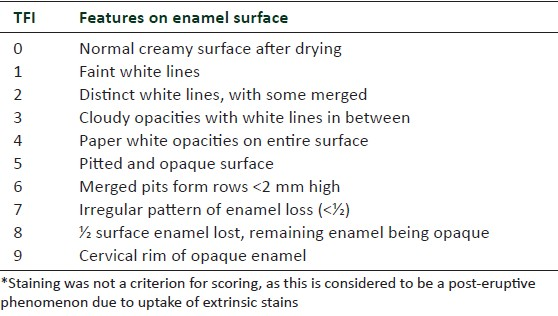
- Fluorosis – TF score for every tooth
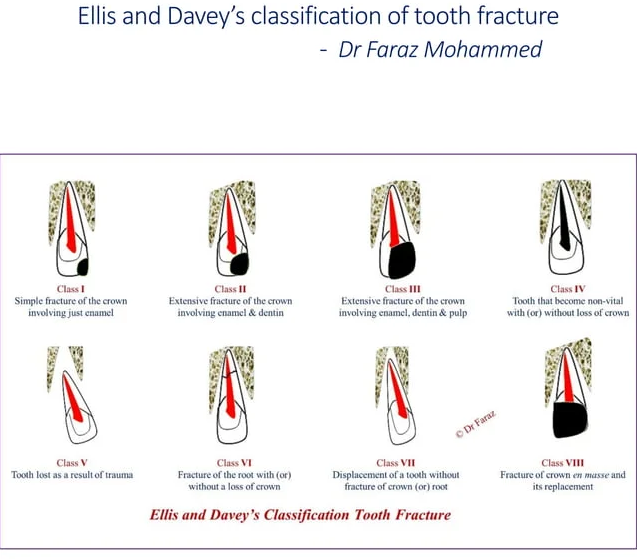
Tooth fracture classification
Periodontal assessment
Gingiva:
- Color: Pink, physiologic pigmentation, red, cyanotic
- Size: Mild, moderate, severe inflammed
- Shape: Scalloped, rounded, col – if space between 2 teeth
- Consistency: Firm, flabby
- Texture: Stippling on attached gingiva
Oral hygiene:
- Calculus – presence of supra or subgingival calculus
- Plaque seen with naked eye
Gingival index by Loe and Silness 1963:
- Facial and lingual surface of index teeth: 16, 11, 24 and 36, 31, 44
- Rate:
- 0 = Normal
- 1 = minimal inflammation, erythema, no bleeding
- 2 = Bleed on probing
- 3 = Spontaneous bleeding
- Find mean score
- GI score:
- 0-1 = Mild
- 1-2 = Moderate
- 2-3 = Severe
Periodontal index by Turesky et al modified Quigley Hein 1970:
Index teeth and disclosing tablet
- 0 = No plaque
- 1 = Flecks at cervical margin
- 2 = Thin continuous band at cervical margin
- 3 = Band wider than 1mm, < 1/3 of crown
- 4 = Plaque < 2/3 of crown
- 5 = Plaque > 2/3 of crown
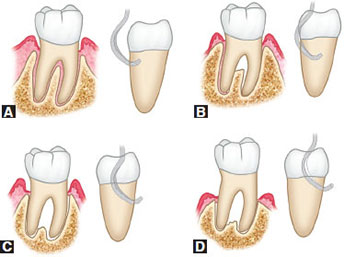
Furcation involvement – Glickman classification 1953
- Grade 1 – Incipient, pocket formation into furcation fluting, interradicular bone intact
- Grade 2 – Moderate loss of interradicular bone but not through and through
- Grade 3 – Probe goes through and through, orifice occluded by gingival tissue
- Grade 4 – Exposed furcation
Periodontal charting:
- Draw continuous line of free gingival margin – facial and lingual
- Draw interrupted line indicating bone level on facial side
- Record 6 point pocket depth
- Record tooth mobility
- Record missing teeth (X), open contacts(//) and how many mm, overhang restorations (V)
- Calculate clinical attachment loss (CAL): Gingival recession + pocket depth
- 1-2mm = Mild
- 3-4mm = Moderate
- > 5mm = Severe
- Localized: < 30% of sites
- Generalized: > 30% of sites
Orthodontic assessment
- A-P: Molar, canine, incisor relationship – Class I, II, III
- Vertical: Open bite, overbite – deep or open
- Transverse:
- Crossbite anterior or posterior
- Midlines
- Crowding or spacing
- Rotation or displacement
- Proclination
- Upper and lower arch form – Normal, V shape, square shape
Investigations
- Radiological – describing a x-ray:
- Name and age of patient
- Date when the x-ray was taken
- Quality
- Teeth present
- Dental age and why
- Radiolucent/radiopaque lesions
- Microbiological
- Histopathological
- Study model
- Diet chart
- Plaque score
- BMI
Diagnosis
- Summarize findings: eg. A 5 year old African male with early childhood caries, dentoalveolar abscess secondary to extensive decay on 55, irreversible pulpitis 85 and 75, and occlusal caries on 54, 64, 84, 74
- For periodontal diagnosis: Severity – extent – diagnosis, eg:
- Mild – localized – chronic periodontitis
- Moderate – generalized – plaque induced gingivitis secondary to orthodontic treatment and mouth breathing
Prognosis for periodontology
1. Excellent prognosis:
- No bone loss
- Excellent gingival condition
- Good patient co-operation
- No systemic/environmental factors
2. Good prognosis:
- Adequate remaining bone support
- Adequate control of etiologic factors and maintainable dentition
- Adequate patient co-operation
- No systemic/environmental factors or well controlled
3. Fair prognosis:
- Less than adequate bone support
- Some tooth mobility
- Grade 1 furcation
- Adequate maintenance possible
- Acceptable patient co-operation
- Presence of limited systemic/environmental factors
4. Poor prognosis:
- Moderate-advanced bone loss
- Tooth mobility
- Grade 1 or 2 furcation involvement
- Doubtful patient co-operation
- Presence of systemic/environmental factors
5. Questionable prognosis:
- Advanced bone loss
- Tooth mobility
- Grade 2 or 3 furcation involvement
- Inaccessible areas
- Systemic/environmental factors
6. Hopeless prognosis:
- Advanced bone loss
- Extraction indicated
- Non maintainable areas
- Uncontrolled systemic/environmental factors
NB: Factors affecting prognosis:
- Diagnosis: Disease severity, plaque and calculus
- Systemic factors: DM, puberty, genetic
- Occlusal factors
- Prosthetic and restorative factors: Caries, teeth vitality, abutment selection, subgingival restorations, fixed or removable prosthesis
- Patient factors: Compliance, co-operation, attitude
- Environmental factors: Smoking, alcohol. bruxism
Treatment objectives
- To control infection and relieve pain and discomfort
- To modify attitude to dental care, and behavior to dental treatment
- To improve oral hygiene
- To restore integrity and function of the dentition
- To achieve cariostasis
- To improve esthetics and correct malocclusion
- To maintain a healthy oral cavity
- Diet planning
Treatment planning
- Oral hygiene instruction (OHI)
- Emergency phase: Systemic diseases, infections
- Etiological phase: Plaque and calculus
- Restorative phase: Filling, RCT, Prosthetic replacement
- Maintenance phase: Recall and review
Periodontal treatment planning
- Preliminary phase: Systemic disease, infections, OHI
- Etiological phase: FMS, root planing, fluoride treatment, cavity prep and filling
- Surgical phase: Disimpaction, gingivectomy, implants, open flap debridement, GTR, furcationplasty
- Restorative phase: Crown, bridge, crown for implant
- Supportive periodontal therapy/maintenance phase: Review after 2 weeks
- High risk – recall every 3 months
- Moderate risk – recall every 6 months
- Low risk – recall every year
Pediatric treatment planning
- Systemic phase – Stabilize chronic illness before dental treatment
- Emergency phase – Antimicrobials
- Preventive phase – OHI, behavior management, fluoride application, diet counselling, pit and fissure sealants
- Preparatory phase – Oral prophylaxis, caries control if multiple lesions, preventive orthodontic consultation
- Corrective phase – Restorations, prosthetic replacement, extractions, Interceptive orthodontic consultation
- Maintenance phase – Recall and review, 3-6 months
- Significance of oral prophylaxis:
- Introduction to dental environment/behavior management
- Oral hygiene education
- Uncover carious lesion covered in plaque
- Healthy gingiva

1 thought on “History, clinical examination and treatment planning”
Comments are closed.