| Pemphigus vulgaris | Mucous membrane pemphigoid | |
| Etiology Target proteins | – Autoimmune reaction – Intercellular keratinocyte protein (desmoglein 3) destroyed by auto antibodies | – Autoimmune reaction to basement membrane proteins: – Lamina 5 – BP 180 |
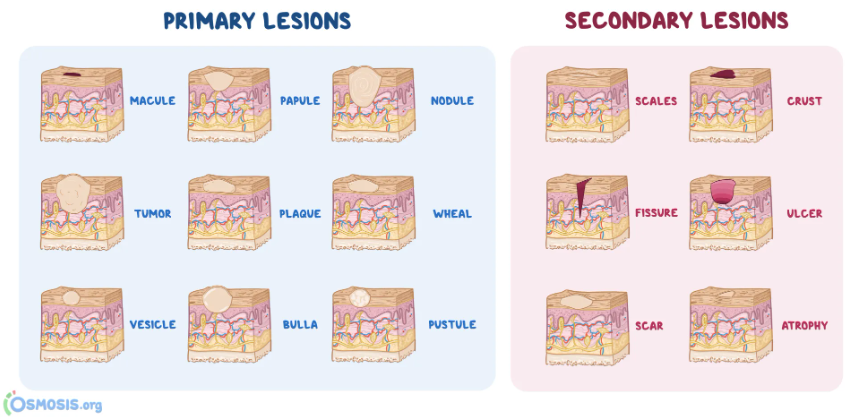
| Clinical | Intraepithelial blisters | Subepithelial blisters |
| Site | – Oral mucosa – Skin – Mucosa | – Oral mucosa – Conjunctiva – Skin rarely |
| Histology | – Intraepithelial clefting – Loss of desmosomal contacts therefore free floating acantholytic Tzanck cells | – Subepithelial clefting – Chronic inflammatory infiltrate |
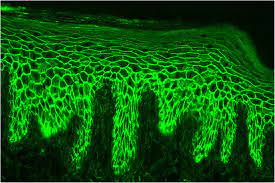
| Direct immunofluorescence testing | Circulating auto IgG | No circulating auto IgG |
Pemphigus vulgaris
- Autoimmune blistering disorder
- Results in loss of integrity of intercellular attachments within epidermis and mucosal epithelium
Subtypes:
- P. Vulgaris (common)
- P. Vegetans (wart like)
- P. Foliaceus (flower like)
- P. Erythematosus (reddened)
Nikolsky’s sign: Positive – stroke mucosa gently, vesicle or bulla appears
Management: Corticosteroids + Azathioprine + Cyclophosphamide
Prognosis: Good. Fatal if untreated
Mucous membrane pemphigoid
- Autoimmune blistering disorder
- Results in loss of integrity of dermal-epidermal junctions
- Affects oral tissues in 30% of cases
- More severe
Management: Corticosteroids
Prognosis: Fair
Differential diagnosis:
- Erythematous lichen planus
- Linear IgA disease
- Discoid lupus erythematous
- Contact allergy