- Kaposi sarcoma (KS) is an indolent angio-proliferative spindle-cell tumor derived from endothelial and immune cells infected with human herpes virus type 8 (HHV-8)[1]
- It is a multifocal neoplasm
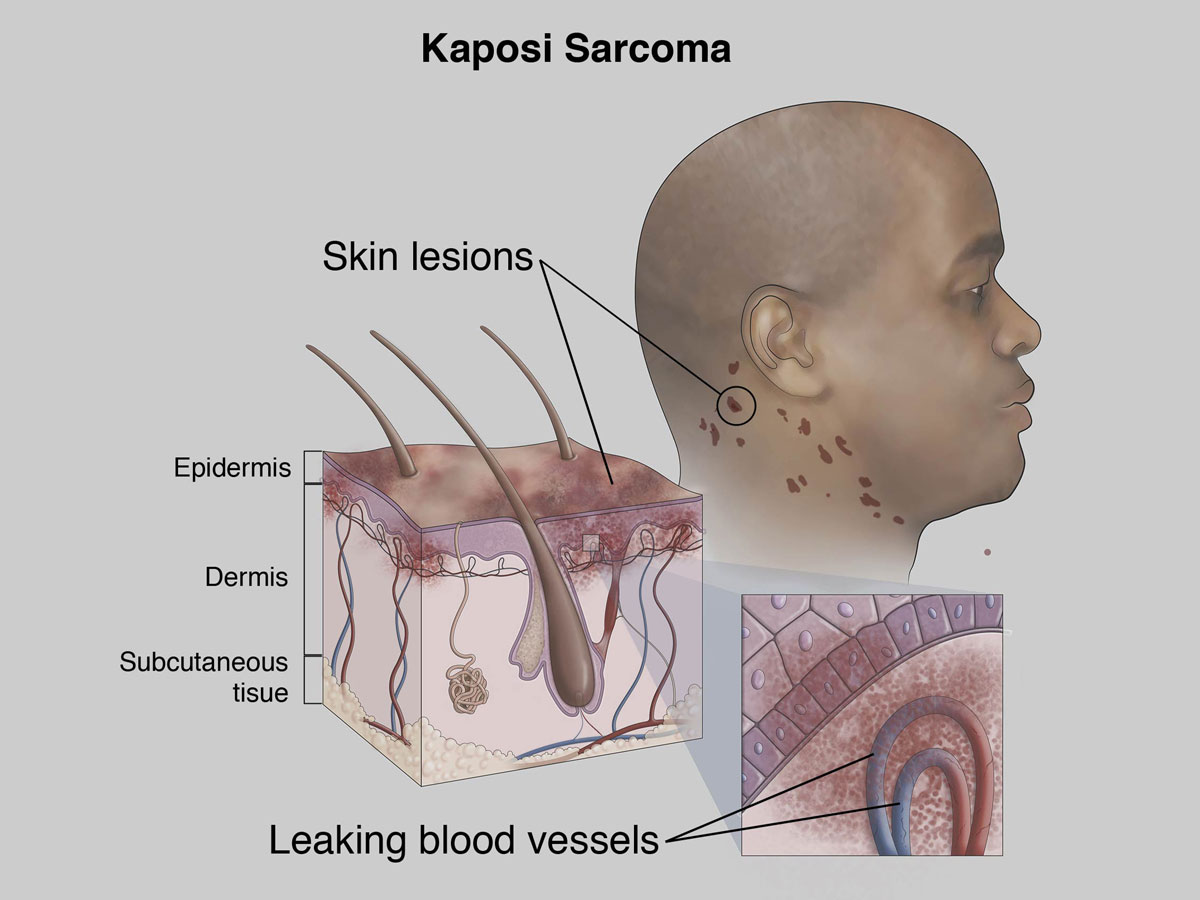
- This is a systemic angiomatosis of malignant evolution which is primarily manifested as multiple vascular nodules in the skin and the organs
- It was first described by Moritz Kaposi, a Hungarian dermatologist in 1872[2]
- It is the most common malignancy in HIV patients
- It is identified as AIDS defining illness
- Etiology:
- HHV8
- Sustained by cytokines and growth factors
- It leads to angioproliferation especially in skin.
- HIV is a predisposing factor to KS.
- It spreads mainly through saliva, such as during sexual contact or in interactions between a mother and child.
- People with healthy immune systems can carry the virus without any problems. But it triggers cancers in people with weakened immune systems
- Pathology:
- HHV-8 invades endothelial cells causing lytic and/or latent infection of the spindle shaped endothelial cells
- Endothelial cells infected with HHV8 undergo altered lymphatic differentiation and manufacture cytokines creating a favorable environment for angiogenesis
- Spread to viscera by dissemination of the involved lymph nodes
- Epidemiology and survival rate:
- It occurs more in men.
- HIV-1 associated Kaposi’s sarcoma has a high occurrence in homosexual men of over 30%. Overall, almost 75% of people who have KS live at least 5 years after diagnosis. If the cancer hasn’t spread, about 82% live at least 5 more years. In people whose cancer has spread to nearby areas, the 5-year survival rate is 60%. The rate is 38% if the cancer has spread farther away
- Origin: Endothelial cells
- Clinical:
- Early lesion – Blue flat macule
- Late lesion – Nodular red blue mass
- Types:
| Epidemiology | Age | Site | Prognosis | |
| Classical | Mediterranean | Old men | Skin Lower extremities | Fair prognosis |
| Endemic | Africa | Children and adults | Skin Extremities | Fair prognosis |
| Immunodeficiency | HIV and transplant patients | Young adults | Skin Mucosa Internal organs | Poor prognosis |
- Diagnosis:
- P24 ELISA
- Viral load
- CD4 count
- CD4 : CD8
- PCR
- HHV8 immunohistochemistry
- Histology: Neoplastic proliferation of endothelial cell origin
- Management:
- The chemotherapy most commonly used for KS is Interferon alpha with didanosine for slowly progressive disease.
- Radiation therapy-for skin lesions.
- In AIDS-related Kaposi’s sarcoma, the first step in treatment is to start or switch to an antiviral drug (ART) combination that will reduce the amount of the virus causing AIDS.
- EG. Chemotherapeutic drugs (Doxorubicin and paclitaxel) with ART.
- Although, KS remains to be controlled than cured.
- Sclerotherapy eg alcohol, propanol, Vinca-alkaloids
- Prevention:
- There’s no vaccine to protect against HHV-8.
- Avoid unprotected sex.
- Avoid injecting drugs with used needles.
- Medications called pre-exposure prophylaxis can also make you less likely to get HIV.
- If you have HIV, antiretroviral therapy (ART) should prevent KS, especially if you start it when your CD4 count is still high. If you’ve had an organ transplant, some anti-rejection drugs can also lower your chance of getting KS

4 thoughts on “Kaposi Sarcoma”
Comments are closed.