Techniques of administrating LA
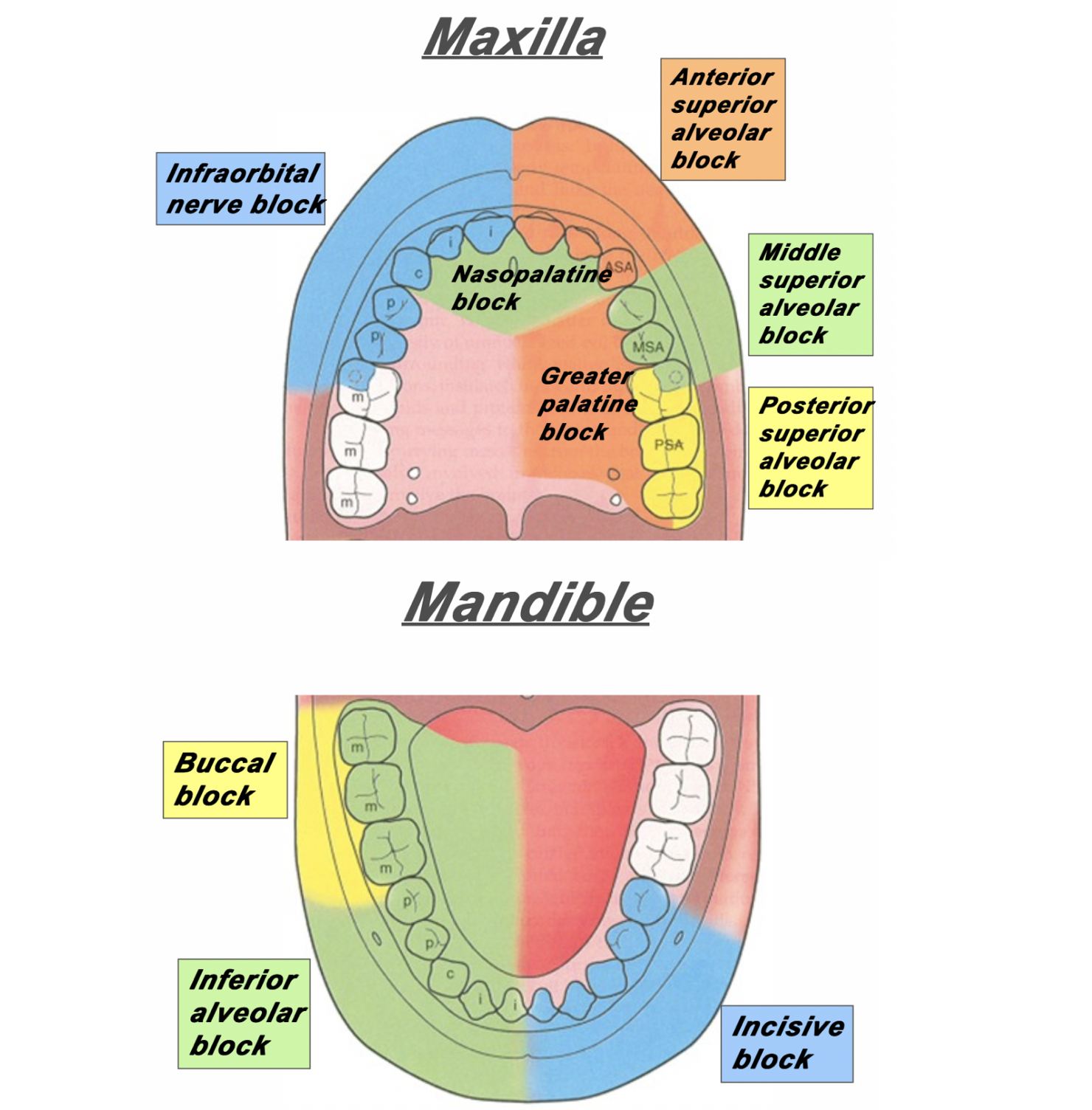
1. Inferior alveolar nerve block: Mandibular posterior teeth
- Between pterygomandibular raphe and coronoid notch (feel with thumb)
- Insert from contralateral side, 1cm above occlusal plane
- Contact bone, withdraw slightly and give LA
2. Mental nerve block: Mandibular anterior teeth
- Between 1st and 2nd premolar
3. Anterior, middle, posterior superior alveolar nerve block: Maxillary teeth
- At junction of mucobuccal fold
4. Greater palatine nerve block: Maxillary posterior teeth
- In front of 1st molar at junction of vertical and horizontal hard palate
- Withdraw after contacting bone
5. Nasopalatine block: Maxillary anterior teeth
- Insert in incisive papilla
6. Infiltration: Picture
- At mucogingival level
7. Buccal Infiltration: Picture
- Parallel to occlusal plane
- Distal to 2nd molar
8. Intrapapillary: Picture
9. Intraligamentary (supplemental): Picture
10. Intrapulpal (supplemental): Picture
11. Intraosseous (supplemental): Picture
12. Gow-Gates technique: Video
13. Vazirani-Akinosi technique: Video
Calculating LA dosage
Use the app Dental Drugs (App store, Play store) to quickly refer for prescribing medications, calculating maximum anesthetic dosages or recalling common treatment protocols in practice
Desirable properties of LA
- Non irritant
- Reversible effect
- Long enough duration for procedure
- Low toxicity
- Fast onset of action
- Potent
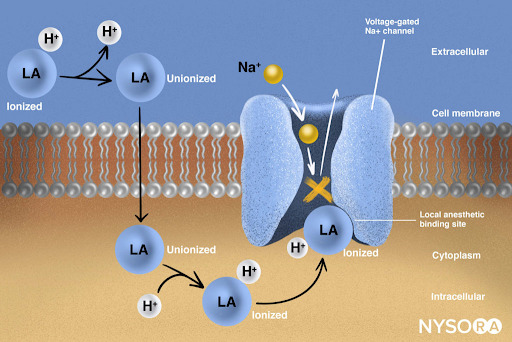
Mechanism of action of LA
LA = Tertiary amine base [B] + Water soluble hydrochloride [B.HCl]
- Injected into tissues
- Base liberated in alkaline pH of tissues
B.HCl + HCO3 = B + H2CO3 + Cl
- Base diffuses through nerve sheath into axoplasm and partially ionizes
B + H+ = BH+
- Ionized form of BH+ enters sodium channel from interior of nerve and combines with a specific receptor in the channel to block sodium influx into the nerve and therefore prevent action potential initiation
BH+ + Receptor = Block sodium influx
Structure of LA
Aromatic group – Intermediate bond (amide/esters)- Tertiary amine

Amides:
- Lignocaine
- Prilocaine – metabolism in liver and lungs. Primary product of metabolism is ortho-Toluidine – associated with methemoglobinemia
- Mepivacaine
- Bupivacaine
Esters:
- Cocaine – Only cocaine causes vasoconstriction
- Procaine – used in case of drug induced arteriospasm. Procaine broken down to PABA – associated with allergic reaction.
- Amethocaine
- Chloroprocaine
Factors affecting LA action
1. pKa (physiologic pH): ↓ pKa leads to faster onset of action as ↑ molecules diffuse through the nerve sheath
2. Lipid solubility: ↑ lipid solubility leads to ↑ potency and therefore block conductions at low concentration
3. Protein binding: ↑ protein binding leads to ↑ duration of action as it firmly attaches to proteins at receptor sites
4. Non nervous tissue diffusibility: ↑ diffusibility leads to slower time of onset
5. Vasodilator activity: ↑ vasodilator activity leads to ↑ blood flow to region and therefore ↑ removal of anesthetic molecules and so ↓ potency and duration
6. Tachyphylaxis: ↑ tolerance when injected repeatedly. Mop up of HCO3, alkaline pH of tissues not sustained
7. Infection: Acidic pH therefore prevent ready formation of free base
Contents of LA
| Local anesthetic agent | Lignocaine HCL | Block nerve conduction |
| Vasoconstrictor | Epinephrine | – Increase duration by decreasing absorption of LA – Control bleeding – Prevent systemic toxicity |
| Reducing agent | Sodium metabisulphite | Antioxidant |
| Preservative | Methylparaben | Bacteriostatic and antioxidant |
| Isotonic solution | Sodium chloride or Ringer’s solution | – |
| Fungicide | Thymol | – |
| Diluting Agent | Distilled water | – |
| To adjust pH | Sodium hydroxide | – |
| Nitrogen bubble | 1-2mm in diameter | To prevent oxygen from being trapped in the cartridge and potentially destroying the Vasopressor or vasoconstrictor |
Pharmacokinetics of LA
1. Uptake:
- LA causes vasodilation and increased uptake into circulation
- Esters cause more vasodilation
- Procaine used in case of drug induced arteriospasm
- Only cocaine causes vasoconstriction
2. IV of LA:
- May cause increased toxicity/adverse effect
- Used to treat ventricular dysrhythmias
- Local and systemic toxicity effects:

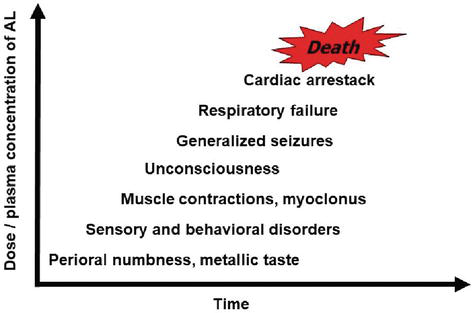
3. Toxicity: Balance between absorption into circulation and rate of elimination from circulation
4. LA crosses blood brain barrier (BBB) and placental barrier
5. Esters metabolized by pseudocholinesterase
- Atypical pseudocholinesterase – cannot metabolize esters – increase toxicity
- Pseudocholinesterase also metabolize succinylcholine – therefore atypical pseudocholinesterase associated with difficult general anesthesia (sleep apnea). Succinylcholine used to cause short term paralysis as part of GA
- Procaine broken down to PABA – associated with allergic reaction
6. Amides metabolized in liver
- Liver perfusion and function important to determine rate of amide elimination
- Liver cirrhosis, hypotension and congestive heart failure – reduce rate of elimination and therefore increase toxicity
- Prilocaine metabolism in liver and lungs. Primary product of metabolism is ortho-Toluidine – associated with methemoglobinemia
Contraindications of LA
| Absolute | LA allergy | Eg. to esters | Give amide |
| Absolute | Sulfur allergy | Avoid articaine | Give non sulfur containing LA |
| Absolute | Bisulfite allergy | Avoid LA with vasoconstrictor | Give LA with no vasoconstrictor |
| Relative | Atypical pseudocholinesterase | Avoid esters | Give amide |
| Relative | Methemoglobinemia | Avoid articaine and prilocaine | Give other LA |
| ASA (III-IV) | Significant liver dysfunction | Avoid amides | Give esters judicially |
| ASA (III-IV) | Significant renal damage | Avoid amides and esters | Give LA judicially |
| ASA (III-IV) | Significant CVD | Avoid high concentration of vasoconstrictor | Give LA with epinephrine concentration 1:100,000 or 1:200,000 |
| ASA (III-IV) | Clinical hyperthyroidism | Avoid high concentration of vasoconstrictor | Give LA with epinephrine concentration 1:100,000 or 1:200,000 |

1 thought on “Local Anesthesia”
Comments are closed.