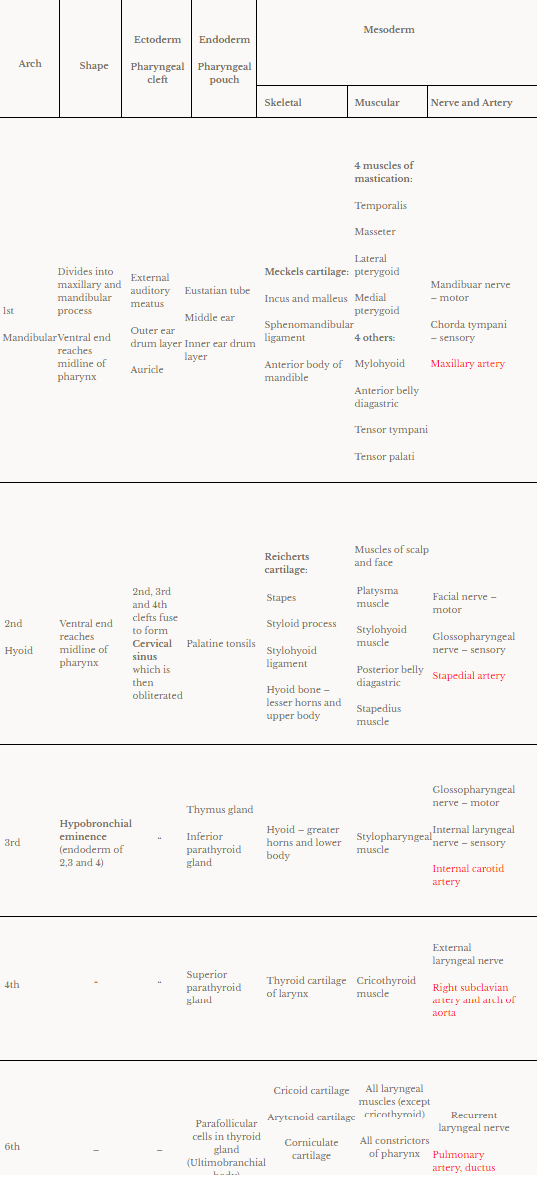
Mesoderm – Cartilagenous bar (forms cartilage, ligaments and bones)
Mesoderm – Striated muscle (special viceral muscle of head and neck)
Aortic arch artery
Own nerve (motor + posttrematic sensory)
Next arch’s nerve (pretrematic sensory)
NB: 5th arch disappears
Derivatives of the arches:
Ectoderm, endoderm, mesoderm derivatives and shape of each pharyngeal arch:
Anomalies:
Branchial cyst – along anterior border of sternocleidomastoid muscle due to failure of cervical sinus to obliterate
Branchial sinus – Branchial cyst opens into skin by narrow canal
Branchial fistula – Branchial cyst opens into lumen of pharynx
Duplication of external auditory meatus – 1st branchial anomaly
Note: If left untreated, may become repeatedly infected and inflamed. Recurrent inflammation makes surgical resection more difficult. Excellent prognosis if lesion is completely resected.
Continuation of external iliac artery ⇒ Femoral artery ⇒ descends infront of thigh ⇒ curves to join sciatic artery backwards to form Poplitial artery
Continuation of Internal iliac artery ⇒ Called sciatic artery ⇒ descends in back of lower limb ⇒ to sole of foot ⇒ degenerates to form Inferior gluteal artery, peroneal artery ETC
EIA and IIA anastomose to form anterior and posterior tibial arteries
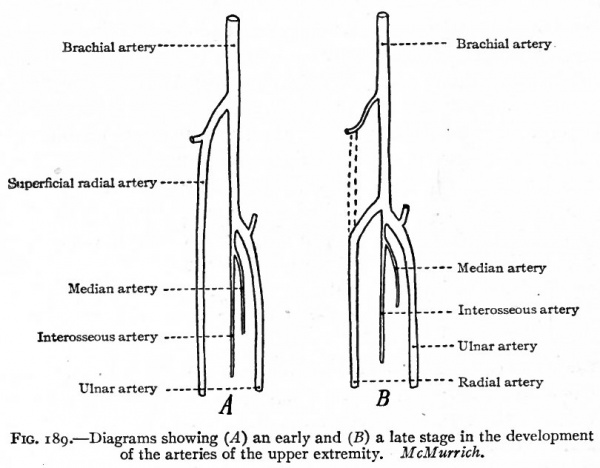
Development of arteries in upper limb:
7th cervical intersegmental artery ⇒ Subclavian a. ⇒ Axillary a. ⇒ Brachial a. ⇒ Ulnar and Radial a. ⇒ give superficial and deep palmer arches
NB: Brachial a. also gives another branch called anterior interosseous artery. Anterior interosseous artery is replaced by median artery which is replaced by ulnar artery
Fuse to form single heart tube ⇒ endocardium of heart
Splanchnic mesoderm, surrounding endocardium of heart, forms myocardium and epicardium
Intraembryonic coelom forms pericardial cavity
3 constrictions appear in the heart tube, dividing it into 4 dilations:
Bulbus cordis ( and truncus arteriosus)
Primitive ventricle
Primitive atrium
Sinus venosus (and right and left horns receiving veins)
The heart tube grows faster than pericardium
Forms U shape, then S shape heart tube
Internal:
1. Sinus venosus
Opens in primitive atrium by sinoarterial orifice guarded by right and left valves
Derivatives of all parts of the sinus venosus are shown below in red
2. Atria
Development of interarterial septum: 3 sources
1. Septum intermedium of AV (atrioventricular) canal
On wall of AV canal
2 proliferations appear
Ventral endocardial cushion
Dorsal endocardial cushion
Which fuse to form septum intermedium
AV canal divided into right (tricuspid) and left (mitral) canals
2. Septum primum – 1st septum
Sickle shaped – has ventral and dorsal horns
Arises from roof of common atrium, left of sinoarterial orifice
Decends to septum intermedium
Ventral and dorsal horns unite with ventral and dorsal endocardial cushions
Due to crescent shape, gap remains – Ostium primum
Caudal growth of septum primum obliterates ostium primum
Cephalic part of septum primum breaks down to form foramen ostium secondum
3. Septum secondum
Sickle shaped – has ventral and dorsal horns
Arises from roof of common atrium, between septum primum and sinoarterial orifice
Decends to septum intermedium
Ventral and dorsal horns unite with ventral and dorsal endocardial cushions
Due to its crescent shape, gap between septum primum and septum secondum – Foramen Ovale
Foramen ovale closes at birth – fusion of septum primum and secondum to form interarterial septum
NB: Embryological remnant in adult heart:
Fossa ovalis
Limbus – caudal edge of septum secondum
Right and left AV canals are absorbed in corresponding atrium
Common pulmonary vein and its two tributaries are absorbed in wall of left atrium, therefore the 4 pulmonary veins open separately in left atrium
Right atrium
Rough anterior part and auricle – common atrium
Posterior smooth part – Sinus venarum (venosus) and absorbed right AV canal
Left atrium
Auricle – common atrium
Remaining smooth part – Absorbed pulmonary vein and AV canal
Anomalies of interarterial septum:
Premature closure of foramen ovale – Right atria and ventricular hypertrophy, left atria and ventricle underdevelopment
Probe patent foramen ovale – so small, blood cannot pass
Ostium secondum defect – large opening
Cyanosis – Blueish discoloration of skin, due to less O2 in blood
Interarterial septum failed to form – 3 chambers, triocular heart
Anomalies of AV canal
Failure of formation of septum intermedium
Ostium primum defect – failure of closure of ostium primum
Tricuspid atresia – fusion of tricuspid valves – patent foramen ovale – hypertrophy of left ventricle – patent IV (interventricular) foramen – small right ventricle
3. Bulbus cordis
1. Proximal part
Absorbed in primitive ventricle to form common bulboventricular chamber
Forms trabecular part of right ventricle
2. Middle part
Infundibulum of right ventricle
Vestibule of left ventricle
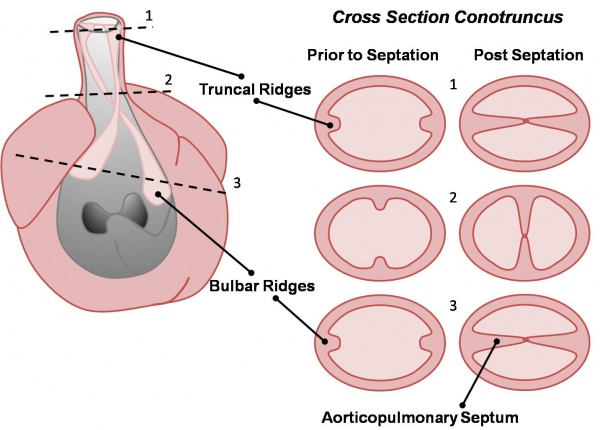
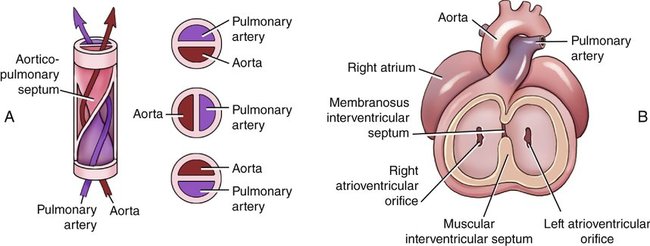
3. Distal part – Divided by spiral septum
Right and left major bulbar cushions develop
Descend to ventricles in a spiral course
Fuse to form aortic pulmonary septum to form pulmonary trunk and ascending aorta
4. Development of IV septum
1. Muscular part:
Arises from floor of bulboventricular chamber
Crescent shape, grows cranially
Anterior horn fuses with ventral root of bulbus cordis
Posterior horn fuses with septum intermedium
2. Membranous part:
Proliferation of:
Right and left major bulbar cushions
Anterior and posterior endocardial cushions
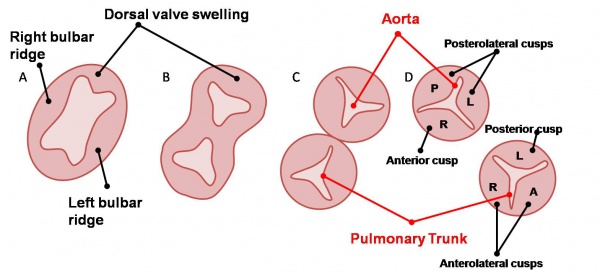
5. Development of aortic and pulmonary semilunar valves
Location: Junction of truncus arteriosus and bulbus cordis
Source:
Right and left major bulbar cushions – fuse to form aortic pulmonary septum
Anterior and posterior minor bulbar cushions – arise perpendicular to above
Before rotation:
Aorta:
1 posterior aortic cusp – from posterior minor bulbar cushion
2 anterolateral aortic cusps – from the major bulbar cushions
Pulmonary trunk:
1 anterior cusp – from anterior minor bulbar cushion
2 posterolateral cusps – from the major bulbar cushions
After rotation of heart to left, the adult cusp postions:
Aorta:
1 anterior cusp
2 posterolateral cusps
Pulmonary trunk:
1 posterior cusp
2 anterolateral cusps
Anomalies of semilunar valves:
Pulmonary stenosis – ductus arteriosus remains open
Aortic stenosis – ductus arteriosus remains open
Anomalies of position of heart:
Dextrocardia – mirror image. If many organs are also mirror images, known as situs inversus totalis
Ectopic cordis – defect in sternum, fails to close in midline, heart exposed to thorax surface
Anomalies of truncus arteriosus:
Fallot’s teratology:
Most common anomaly of heart
Pulmonary stenosis
Cause hypertrophy of right ventricle
Ventricular septal defect
Overriding aorta receives blood from right and left ventricles
Persistent truncus arteriosus – failure to develop AP septum, accompanied by ventricular septal defect and overriding aorta
Transposition of aorta and pulmonary trunk – AP septum runs straight instead of spiral course, aorta opens in right ventricle and pulmonary trunk opens in left ventricle. ductus arteriosus remains open to carry O2 blood to aorta
Made of amnioblasts and somatopleuric layer of extraembryonic mesoderm
The connecting stalk is only made of extraembryonic mesoderm
The amnion cavity obliterates extraembryonic coelom
Functions of amniotic fluid (made from amnioblasts and fetal urine):
Cushions the baby
Develops the suckling reflex
Space for urine discharge
Maintains constant temperature
Antiseptic – cleanses vagina when the water breaks
Allows movement of embryo – muscle development
Bag of waters – dilates cervix gently
Abnormalities:
Oligohydramnios – less amniotic fluid, adhesion of embryo to itsself and the amnion
Polyhydramnios – more amniotic fluid, premature rupture
Umbilical Cord
Tubular sheath of amnion from placenta to umbilicus (naval)
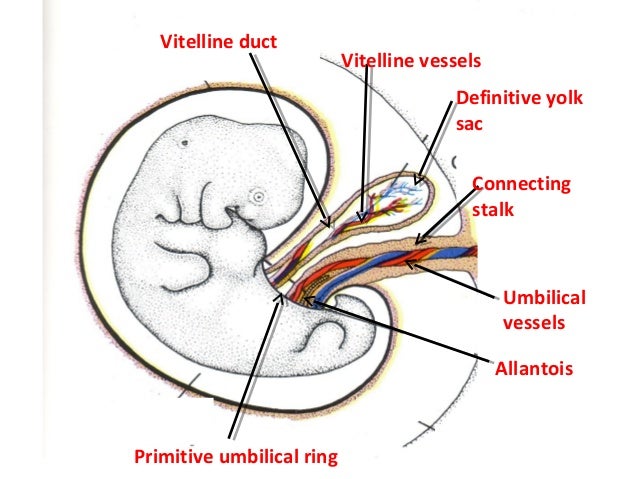
Development of the cord:
1. Primitive umbilical ring – line of reflection between amnion and ectoderm
2. Primitive umbilical cord
Body stalk
Yolk sac
Part of allantois (later in the chapter)
3. Definitive umbilical cord
Wharton’s jelly (mucoid substance from extraembryonic mesoderm)
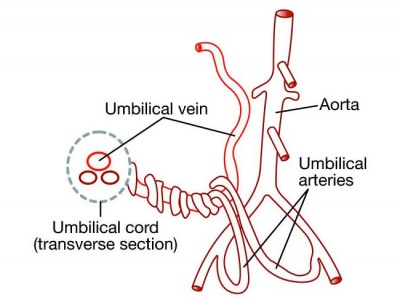
2 umbilical arteries
1 umbilical vein
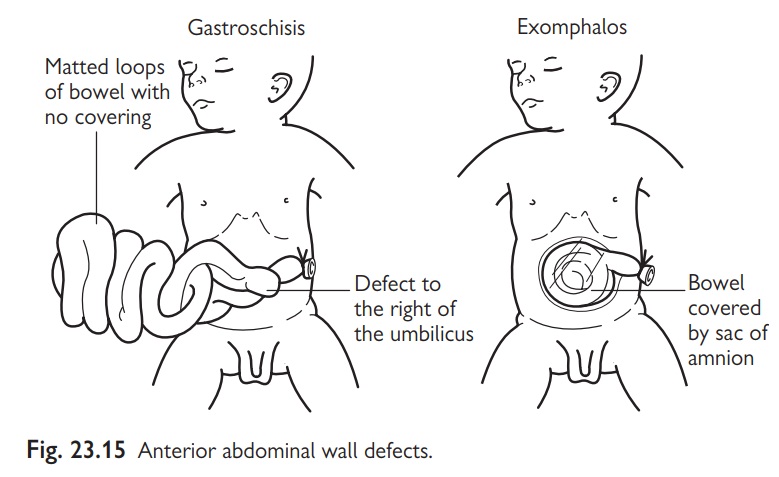
Physiological hernia between 6th and 10th week
Abnormalities:
Short cord
Long cord – can wrap around fetus neck
Exomphalos – failure to reduce physiological umbilical hernia
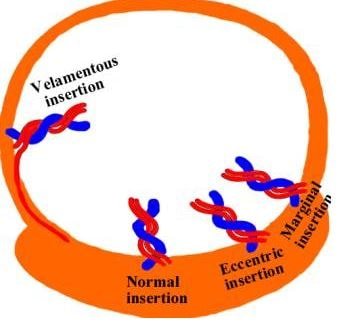
Attachment to placenta can be eccentric, marginal or velamentous (surrounding fetal membranes)
One umbilical artery instead of two
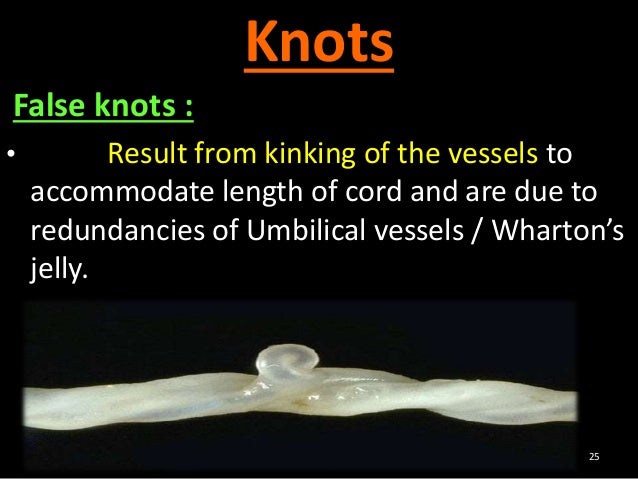
False knots
True knots – dangerous, obstruct blood flow
Two to three umbilical cords
Yolk Sac
1. Primary yolk sac – Heusers membrane
2. Secondary yolk sac – Extraembryonic coelom
3. Folding of embryonic disc – primitive gut and definitive yolk sac
The embryonic disc folds in a cranial-caudal and lateral direction, because the central area of the disc grows more then the periphery. This results in the incorporation of the yolk sac roof into the embryo forming the primitive gut which is divided into foregut, midgut and hindgut.
The part of the yolk sac which was not incorporated is known as definitive yolk sac and is connected to the primitive gut by vitellointestinal duct at the midgut.
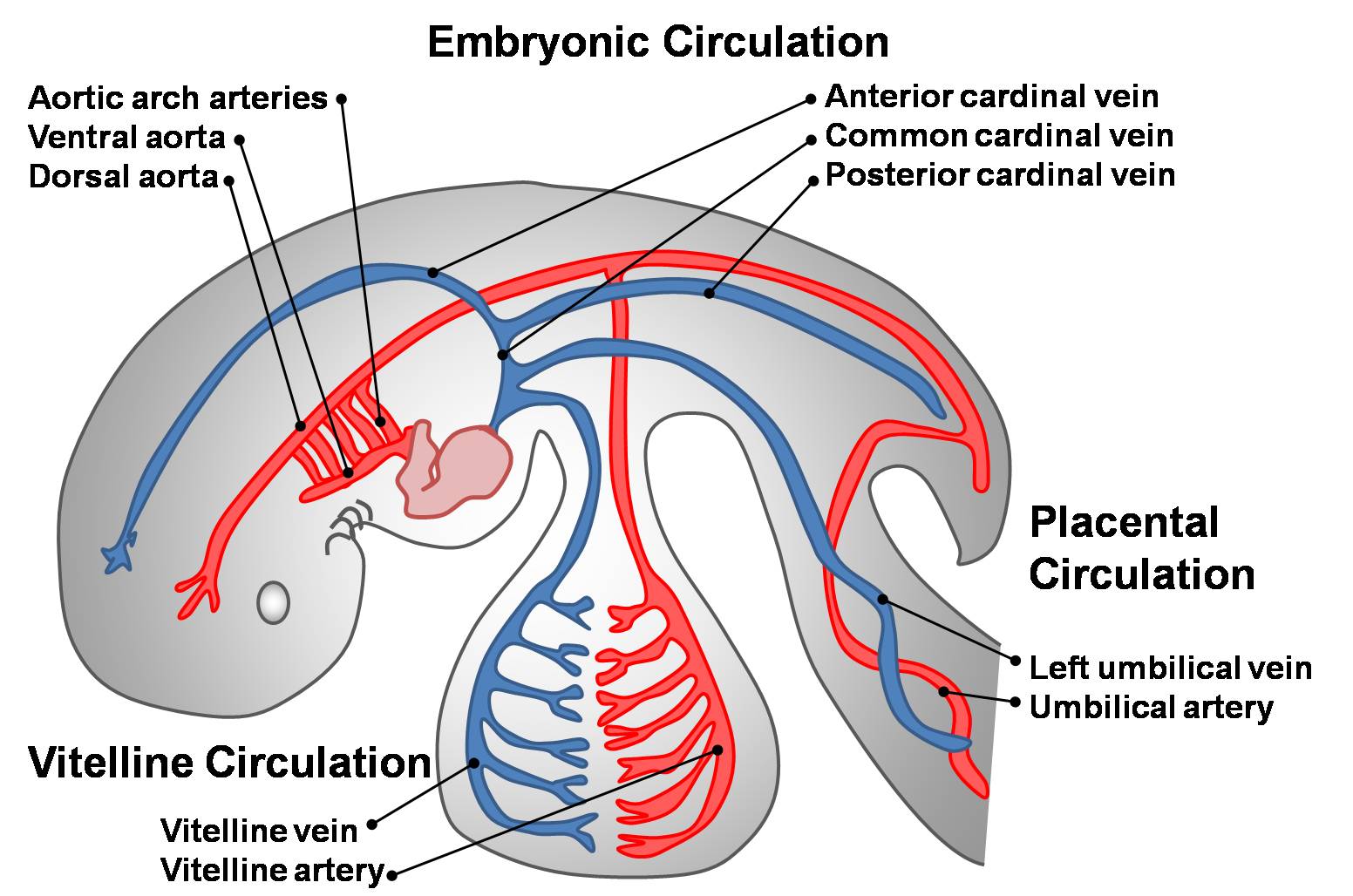
Vitelline vessels – network of vessels develop in splanchnopleuric mesoderm covering the secondary yolk sac
Functions of yolk sac:
Roof forms primitive gut
Caudal end forms allantois
Gives primordial germ cells which migrate to developing gonads
Some vitelline vessels form embryonic vessels
Allantois
Allantoic vessels form the umbilical artery and vein
It’s a tubular invagination of the secondary yolk sac
It has 2 parts:
1. Intraembryonic part: forms urachus which connects urinary bladder to umbilicus. After birth, the urachus is obliterated to form median umbilical ligament
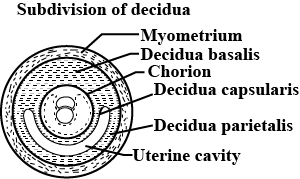
After implantation, the endometrium is known as decidua.
Three types of decidua:
Decidua basalis – forms maternal part of placenta
Decidua capsularis – degenerates
Decidua parietalis – degenerates
The chorionic villi over the embryonic pole remain and develop to form numerous villi. That part is known as chorion frondosum and is the fetus part of placenta.
The remaining part of the chorionic vesicle has no villi and is known as chorion laeve.
Placenta: Chorion frondosum and decidua basalis
Placental barrier: separates fetal and maternal blood and is made of:
1. Early pregnancy
Capillary wall
Extraembryonic mesoderm
Cytotrophoblast
Syncytiotrophoblast
2. Late pregnancy
Capillary wall
Syncytiotrophoblast
Placenta increases in thickness due to villi elongation, intervillus space increases
Placenta increases in diameter due to secondary growth of uterine wall
Functions of placenta:
Nutrition
Respiration
Excretion
Protective
Prevents most microorganisms
Antibodies transmitted
Prevents blood from mixing
5. Secretory
Progesterone
Estrogen (make uterus sensitive to oxytocin hormone)
Gonadotropic hormones
Clinicals:
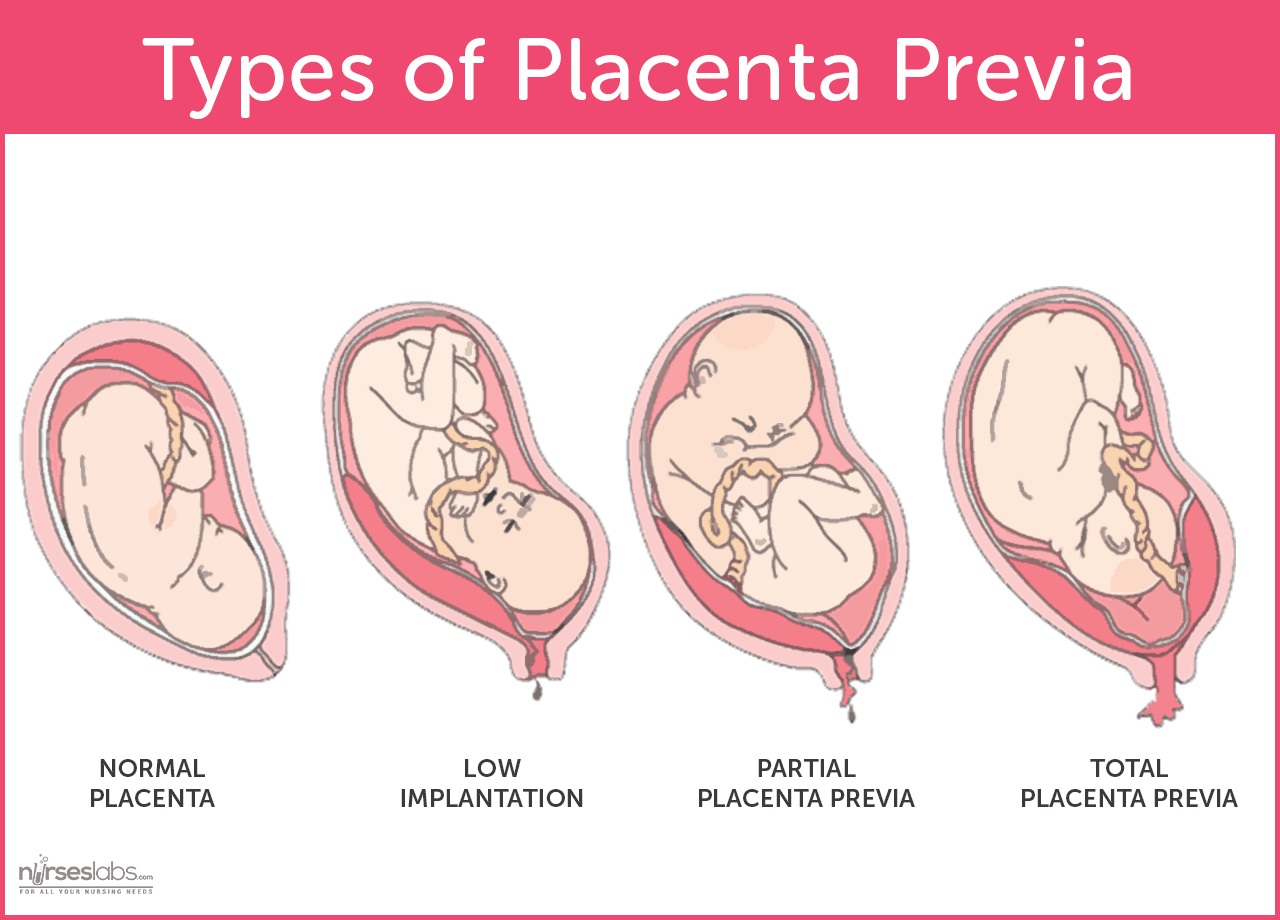
1. Placenta previa – implantation occurs in lower part of uterus
2. Diffuse placenta – placenta lines greater part of uterine cavity
3. Bidiscoid placenta – placenta has 2 disc like equal parts, where each receive a branch from the umbilical artery
4. Accessory placenta – placenta has accessory lobes separate from the main placenta
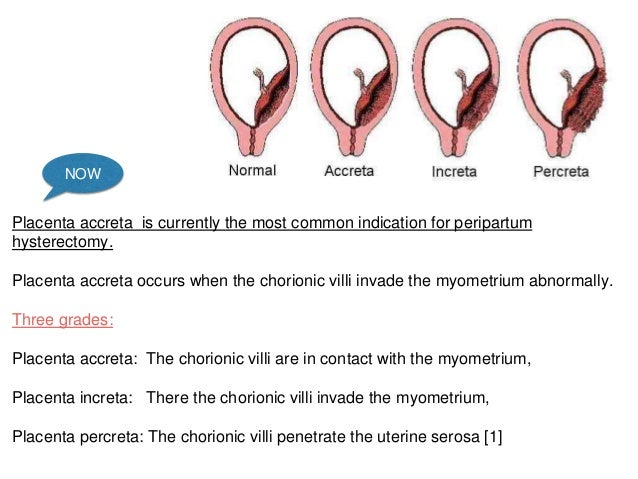
5. Placenta accreta, increta or percreta – placenta too deeply attached to uterus