Origin: Splanchnic mesoderm (of lateral plate mesoderm) infront of buccopharyngeal membrane
External:
- Angiogenetic cells (mesodermal)
- Form 2 endocardial heart tubes
- Fuse to form single heart tube ⇒ endocardium of heart
- Splanchnic mesoderm, surrounding endocardium of heart, forms myocardium and epicardium
- Intraembryonic coelom forms pericardial cavity
- 3 constrictions appear in the heart tube, dividing it into 4 dilations:
- Bulbus cordis ( and truncus arteriosus)
- Primitive ventricle
- Primitive atrium
- Sinus venosus (and right and left horns receiving veins)
- The heart tube grows faster than pericardium
- Forms U shape, then S shape heart tube
Internal:
1. Sinus venosus
Opens in primitive atrium by sinoarterial orifice guarded by right and left valves
Derivatives of all parts of the sinus venosus are shown below in red

2. Atria
Development of interarterial septum: 3 sources
1. Septum intermedium of AV (atrioventricular) canal
- On wall of AV canal
- 2 proliferations appear
- Ventral endocardial cushion
- Dorsal endocardial cushion
- Which fuse to form septum intermedium
- AV canal divided into right (tricuspid) and left (mitral) canals
2. Septum primum – 1st septum
- Sickle shaped – has ventral and dorsal horns
- Arises from roof of common atrium, left of sinoarterial orifice
- Decends to septum intermedium
- Ventral and dorsal horns unite with ventral and dorsal endocardial cushions
- Due to crescent shape, gap remains – Ostium primum
- Caudal growth of septum primum obliterates ostium primum
- Cephalic part of septum primum breaks down to form foramen ostium secondum
3. Septum secondum
- Sickle shaped – has ventral and dorsal horns
- Arises from roof of common atrium, between septum primum and sinoarterial orifice
- Decends to septum intermedium
- Ventral and dorsal horns unite with ventral and dorsal endocardial cushions
- Due to its crescent shape, gap between septum primum and septum secondum – Foramen Ovale
- Foramen ovale closes at birth – fusion of septum primum and secondum to form interarterial septum
NB: Embryological remnant in adult heart:
- Fossa ovalis
- Limbus – caudal edge of septum secondum
Right and left AV canals are absorbed in corresponding atrium
Common pulmonary vein and its two tributaries are absorbed in wall of left atrium, therefore the 4 pulmonary veins open separately in left atrium
Right atrium
Rough anterior part and auricle – common atrium
Posterior smooth part – Sinus venarum (venosus) and absorbed right AV canal
Left atrium
Auricle – common atrium
Remaining smooth part – Absorbed pulmonary vein and AV canal
Anomalies of interarterial septum:
- Premature closure of foramen ovale – Right atria and ventricular hypertrophy, left atria and ventricle underdevelopment
- Probe patent foramen ovale – so small, blood cannot pass
- Ostium secondum defect – large opening
- Cyanosis – Blueish discoloration of skin, due to less O2 in blood
- Interarterial septum failed to form – 3 chambers, triocular heart
Anomalies of AV canal
- Failure of formation of septum intermedium
- Ostium primum defect – failure of closure of ostium primum
- Tricuspid atresia – fusion of tricuspid valves – patent foramen ovale – hypertrophy of left ventricle – patent IV (interventricular) foramen – small right ventricle
3. Bulbus cordis
1. Proximal part
- Absorbed in primitive ventricle to form common bulboventricular chamber
- Forms trabecular part of right ventricle
2. Middle part
- Infundibulum of right ventricle
- Vestibule of left ventricle
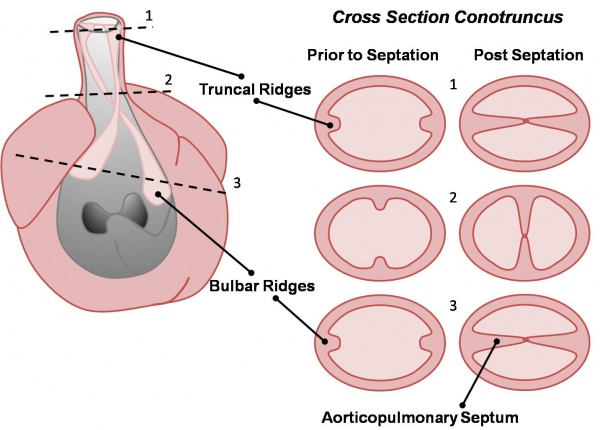
3. Distal part – Divided by spiral septum
- Right and left major bulbar cushions develop
- Descend to ventricles in a spiral course
- Fuse to form aortic pulmonary septum to form pulmonary trunk and ascending aorta
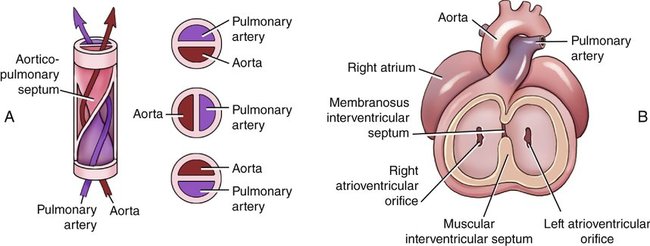
4. Development of IV septum
1. Muscular part:
- Arises from floor of bulboventricular chamber
- Crescent shape, grows cranially
- Anterior horn fuses with ventral root of bulbus cordis
- Posterior horn fuses with septum intermedium
2. Membranous part:
Proliferation of:
- Right and left major bulbar cushions
- Anterior and posterior endocardial cushions

5. Development of aortic and pulmonary semilunar valves
Location: Junction of truncus arteriosus and bulbus cordis
Source:
- Right and left major bulbar cushions – fuse to form aortic pulmonary septum
- Anterior and posterior minor bulbar cushions – arise perpendicular to above
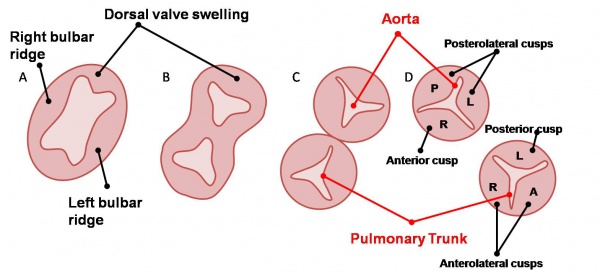
Before rotation:
Aorta:
- 1 posterior aortic cusp – from posterior minor bulbar cushion
- 2 anterolateral aortic cusps – from the major bulbar cushions
Pulmonary trunk:
- 1 anterior cusp – from anterior minor bulbar cushion
- 2 posterolateral cusps – from the major bulbar cushions
After rotation of heart to left, the adult cusp postions:
Aorta:
- 1 anterior cusp
- 2 posterolateral cusps
Pulmonary trunk:
- 1 posterior cusp
- 2 anterolateral cusps
Anomalies of semilunar valves:
- Pulmonary stenosis – ductus arteriosus remains open
- Aortic stenosis – ductus arteriosus remains open
Anomalies of position of heart:
- Dextrocardia – mirror image. If many organs are also mirror images, known as situs inversus totalis
- Ectopic cordis – defect in sternum, fails to close in midline, heart exposed to thorax surface
Anomalies of truncus arteriosus:
- Fallot’s teratology:
- Most common anomaly of heart
- Pulmonary stenosis
- Cause hypertrophy of right ventricle
- Ventricular septal defect
- Overriding aorta receives blood from right and left ventricles

- Persistent truncus arteriosus – failure to develop AP septum, accompanied by ventricular septal defect and overriding aorta
- Transposition of aorta and pulmonary trunk – AP septum runs straight instead of spiral course, aorta opens in right ventricle and pulmonary trunk opens in left ventricle. ductus arteriosus remains open to carry O2 blood to aorta

1 thought on “Development of heart”
Comments are closed.