Liposarcoma
Origin: Adipocytes, rare in head and neck
Clinical: Slow growing mass
Subtypes:
- Well differentiated
- Myxoid
- Round cell
- Pleomorphic
Management:
- Surgical excision with radiation
- Good prognosis
Leiomyosarcoma
Origin: Spindle shaped smooth muscle cells
Resembles fibrosarcoma clinicopathologically, therefore to differentiate in diagnosis
Diagnosis: +ve desmin and +ve actin
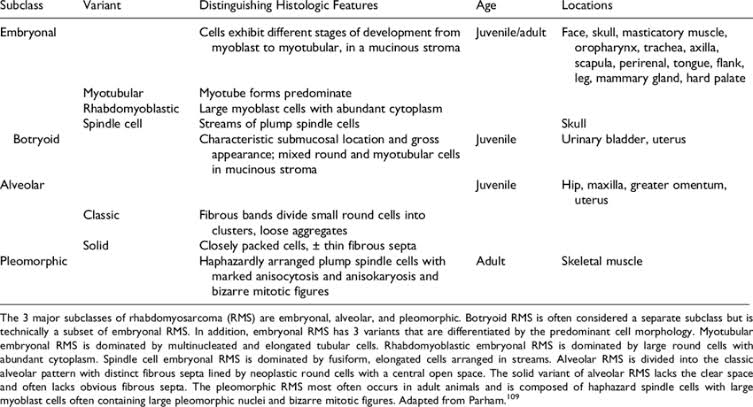
Rhabdomyosarcoma
Origin: Striated muscle
Clinical presentation: Overlying skin is shiny, red, warm, can feel thrill/bruit
Diagnosis: +ve desmin and +ve actin
Management: Surgery, chemotherapy, radiotherapy
Histology:
2 Histological forms:
1. Embryonal:
- In head and neck and GUT
- 4-6 year olds
- Primitive round cells:
- Spindle
- Grape like – botryoid
2. Alveolar:
- Extremities/trunk
- > 10 year olds
Neurofibrosarcoma
Origin: Schwann cells, neural cells
Clinical: Mass causing pain and paresthesia
Histology: Plump spindle cell – arranged in streaming pattern
Diagnosis: If resembles fibrosarcoma, confirm with S-100 staining
Management: Surgery and radiation
