Etiology:
Many contributing risk factors: Genes & environment
Genetic predisposition
Syndromes associated with cleft li and palate
Nutrition: iron, zinc, folic acid, B12 deficiency
Drugs: phenytoin, valproic aid
Alcohol
Maternal smoking
Stress and disturbance during development
Cleft lips: Failure of medial & lateral nasal process to be penetrated by epithelial cells during 6th week in utero.
Cleft palate: Lack of lateral palatal segment fusion – ingrowth of mesoderm – and epithelial breakdown during 8th week in utero
Results in – Mastication, speech, deglutition defect
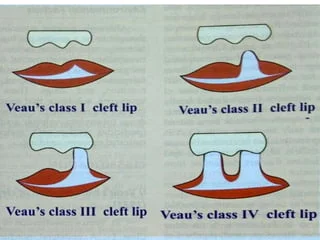
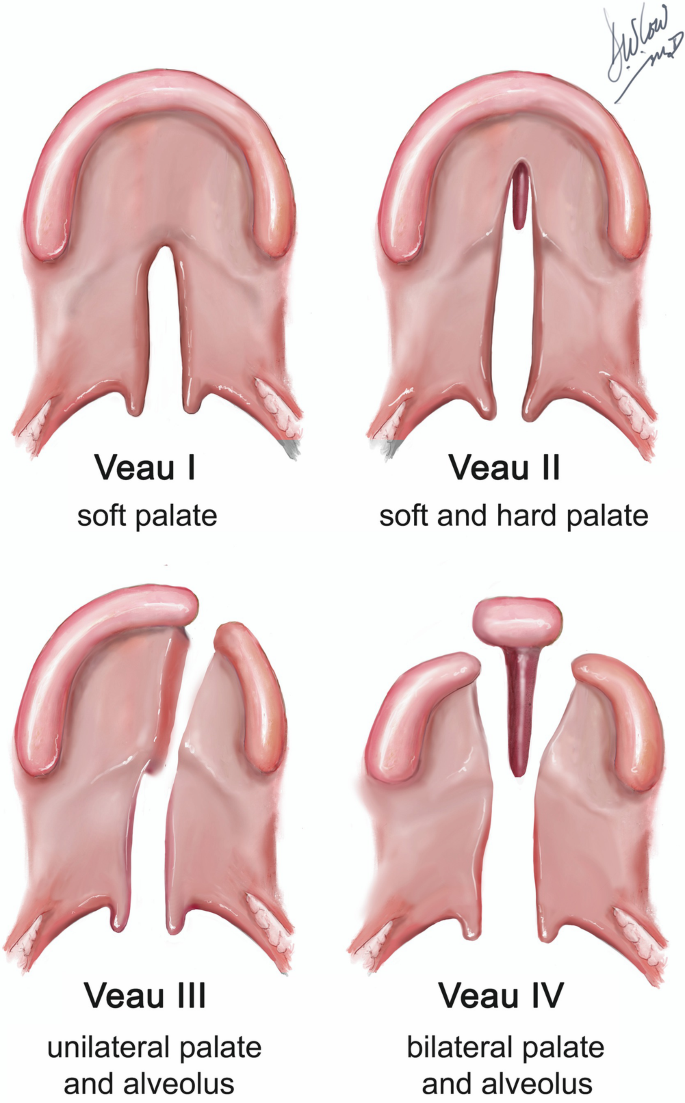
Veau classification:
Cleft lips:
Class I Unilateral notch of vermillion border, not extending to lip Class II Unilateral cleft of lip, not extending to floor of nose Class III Unilateral cleft of lip, extending to floor of nose Class Iv Bilateral cleft of lip
Cleft lips classification table Cleft palate:
Class I Unilateral cleft limited to soft palate Class II Unilateral cleft of hard and soft palate – not extending past incisive foramen (2ry palate) Class III Unilateral cleft extending from uvula to alveolar process Class Iv Bilateral cleft of soft and hard palate
Cleft palate classification table Diagnosis:
Ultrasonography for baby in utero
Management:
Lip surgery
Palate repair – before speech development (1 and half years age)
Speech therapy
Alveolar bone grafting
Orthodontic treatment
Orthognathic surgery (jaw exercise)
NB:
Age 1-3 months – Lip taping and naso-alveolar molding
Age 3 months – Repair of cleft lip
Age 9-12 month – Repair of cleft palate
Age 1-7 years – Orthodontic treatment
Age 7-8 years – Alveolar bone graft
18 years old or skeletal maturity – Midface advancement, continued orthodontic treatment
Rule of 10’s:
Weight ≥ 10 pounds
Hemoglobin ≥ 10 mg/dl
Age ≥ 10 weeks
Associated syndromes:
Van der Woude syndrome
Lower lip pits in patient with cleft lip and palate
AD
Mutations in interferon regulatory factor 6 gene (IRF6)
Associated features:
Hypodontia
Molar incisor hypomineralization
Ankyloglossia (tongue tie)
Syndactyly (webbed fingers)
Picture