Patient positioning when extracting teeth
- Maxillary teeth: 3 inch below shoulder level of operator and 45 degree chair angulation
- Mandibular teeth: At elbow level of operator and 90 degree chair angulation
- 1st, 2nd and 3rd quadrant: Right front of patient
- 4th quadrant anterior teeth: Right front of patient
- 4th quadrant posterior teeth: Behind right side of patient/ just right side
Tooth extraction forceps and elevators
Tooth extraction techniques
Elevator techniques
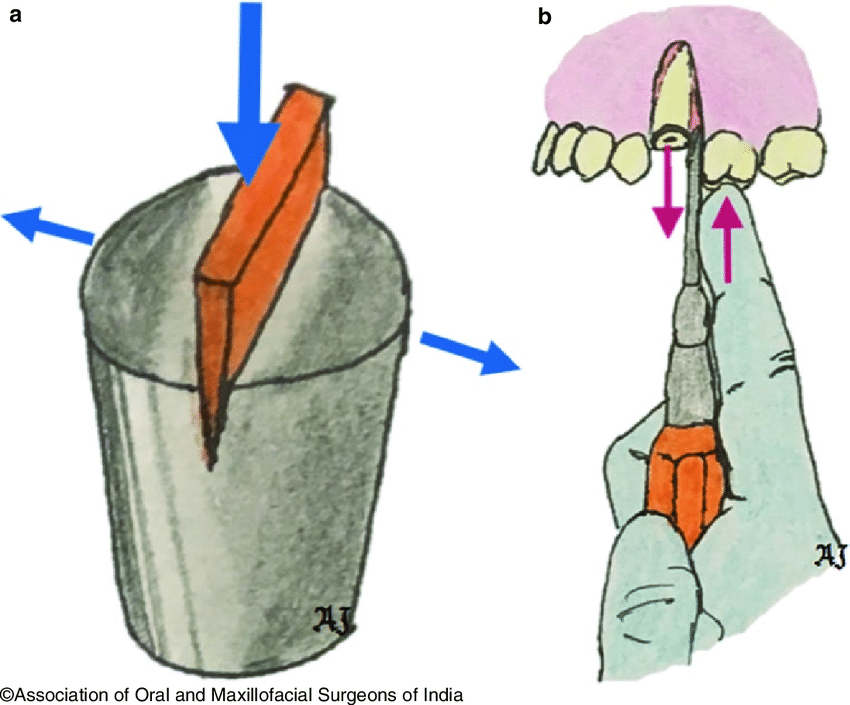
Elevators works on principles of:
- Wedge
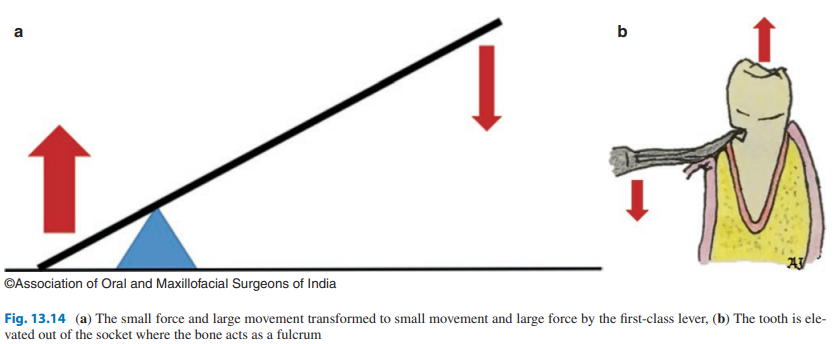
- Lever
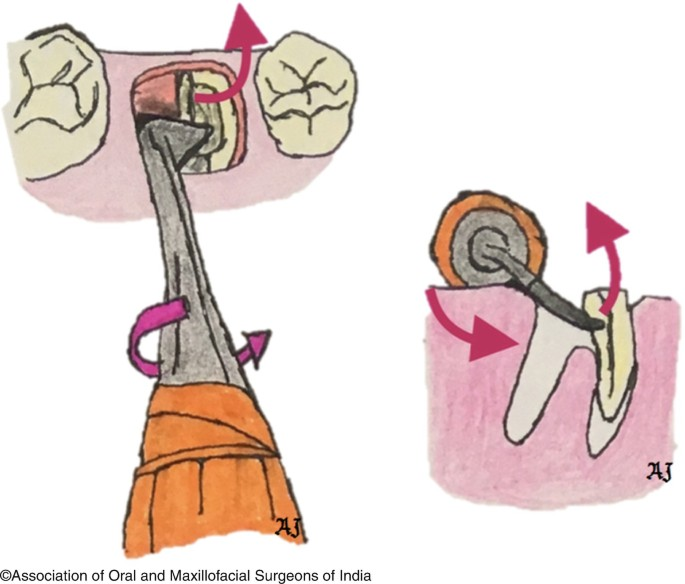
- Wheel and axle
- Combination of the above
1. Wedge principle
2. Lever principle
3. Wheel and axle
Post extraction steps
- Ensure complete tooth and root removal and confirm by showing to patient
- Inspect socket and remove sharp bony margins – if present smoothen with a file
- Compress expanded socket with digital pressure
- Apply pressure pack
- Prescribe analgesics if needed
Post op instructions for patient
- Bite on pressure pack for 30-60 minutes
- Swallow saliva normally
- Do not rinse or spit for 24 hours
- Do not stick finger or tongue at extraction site
- Drink water and fluids normally, do not use straw
- Do not eat until the effects of anesthesia go away
- Eat soft and cold diet
- Apply cold compression/ice pack for swelling
- After 24 hours use salt water rinse
- Avoid smoking for 5 days
Indications
- Gross caries
- Tooth injury and tooth cannot be salvaged
- Tooth in jaw fracture line
- Impacted tooth
- Pre-prosthetic preparation
- Orthodontics
- Supernumerary teeth
- Associated pathology
- Severe periodontal disease
- Retained deciduous teeth
- Patient preference/economic constraints
- Preparation for radiotherapy
Contraindications
Local:
- History of irradiation in that area
- Lack of cooperation or consent from patient
- Lack of proper equipment
- Lack of adequate skill
- Severe infections – control infection first
Systemic:
- Severe metabolic disease – uncontrolled DM, renal disease
- Hepatic dysfunction – decreased coagulative factors
- Coagulopathies – hemophilia, platelet disorder
- History of CVD
- Leukemia
- Pregnancy
- Steroid therapy
NB:
- Avoid extraction during menstruation – risk factor for alveolar osteitis
Complications
a. Complication due to injection technique and anesthetic solution:
- Needle breakage
- Failure to work
- Allergy
- Syncope
- Hematoma if in vessel
b. Complication pre-op
- Lack of cooperation, anxiety
- Poor access – trismus, decreased mouth opening, crowded/malaligned teeth
c. Complications during surgical procedure
- Difficulty in luxation – root dilaceration, curvature, hypercementosis
- Soft tissue injury
- Damage to adjacent teeth
- Fracture of mandible, alveolus or tuberosity
- Fractured instrument – eg. needle
- Tooth/root displacement into maxillary antrum – Caldwell Luc approach to remove
- Loss of extracted tooth or root – stop everything and look for it, can do chest xray
- Nerve injury:
- Neuropraxia – temporary conduction loss
- Axonotmesis – axon and myelin sheath damaged but epineurium, perineurium and endoneurium intact
- Neurotmesis – nerve transection
- Paresthesia – tingling/prickling sensation
- Dysesthesia – abnormal sensation
- Hyperesthesia
- Hypoesthesia
- Anesthesia
- Formation of:
- Phantom limb syndrome
- Anesthesia dolorosa – sense of touch diminished but malfunctioning painful sensation left intact in trigeminal nerve
d. Complications after procedure
- Hemorrhage
- Primary – laceration of artery, surgery done in infected area with granulation tissue
- Reactionary – occurs few hours after surgery , failure of coagulation
- Secondary – 7-10 days after surgery, due to infection + partial division of blood vessel
- Alveolar osteitis
- Infection
- Delayed healing
- Pain

1 thought on “Tooth extraction”
Comments are closed.